Analysis of Components and Effects of Chest Compression Posture using CPR Training System
Volume 9, Issue 2, Page No 17-25, 2024
Author’s Name: Taiki Yamakamia), Akinori Minaduki
View Affiliations
Kushiro Public University, Economics, Minaduki Lab, Kushiro City,085-8585, Japan
a)whom correspondence should be addressed. E-mail: s202103@kpu.kushiro-pu.ac.jp
Adv. Sci. Technol. Eng. Syst. J. 9(2), 17-25 (2024); ![]() DOI: 10.25046/aj090203
DOI: 10.25046/aj090203
Keywords: CPR, CPR Training System, Azure Kinect DK, Body tracking

Export Citations
Cardiopulmonary resuscitation (hereafter CPR) is a life-saving procedure to combat our day-to-day risks of cardiac arrest. However, there are a few citizens who can accurately carry out CPR by encountering the scene of the cardiac arrest of others, and there are many unclear parts on the methods such as the correct attitude of CPR, and the condition which lacks the clear scientific reason becomes a problem. This study aims to investigate the lever arm of CPR (cardiopulmonary resuscitation) by Body tracking using Azure Kinect DK to determine the lever arm of CPR (cardiopulmonary resuscitation) by Body tracking. As a movement toward this goal, this time we analyzed the effect of hand up/down changes in CPR posture on CPR and posture from a clear numerical value of joint angle.
Received: 11 January 2024, Revised: 20 February 2024, Accepted: 21 February 2024, Published Online: 23 March 2024
1. Introduction
Cardiopulmonary resuscitation (hereafter CPR) is a life-saving procedure to combat our day-to-day risks of cardiac arrest. However, there are a few citizens who can accurately carry out CPR by encountering the scene of the cardiac arrest of others, and there are many unclear parts on the methods such as the correct attitude of CPR, and the condition which lacks the clear scientific reason becomes a problem. CPR Training Posture Analysis Simulator (hereafter CPR Training System) developed in this study visualized the posture of the upper and lower extremities during chest compression in CPR from two frontal and lateral directions using Azure Kinect DK. The development of a posture-conscious CPR training system allowed objective assessment of posture and compression (including decompression) during chest compressions [1],[2]. CPR training system is aimed at the public to disseminate the practical education and training of CPR, and at the same time, to pursue the proper postural shape of CPR position with many unknown parts based on the training record data accumulated through the experiment.
As an approach to elucidate the appropriate posture to perform chest compressions during CPR, which has not been elucidated in previous studies, CPR posture is divided into parts, and the appropriate posture with scientific evidence is analyzed for each part. In this study, we analyzed the effects of CPR postural hand placement and the relation between CPR postures and the number of compressions and muscle strength and muscle mass.
2. Current Status of the Scientific Basis for CPR Attitudes
Currently, it is recommended as an appropriate attitude for CPR by JRC Resuscitation Guideline (Medical Shoin) [3], which is supervised by the Japanese Resuscitation Council, as shown in Figure 1.
Some of the methods of the guideline include those with less certainty of the scientific basis, and the appropriate attitude of CPR remains to be elucidated.
3. Developing NUI Applications for CPR Training
Azure Kinect DK (Kinect) used as an input-sensing sensor device for postural changes in the body during CPR training is an input sensor device for NUI (Natural User Interface connected to Windows PC [4]. Extracting postural movements (shapes; kata) during CPR training and developing a decision-algorithm requires that the entire body is input-detected and user-interfaced when performing CPR. Therefore, in this study, a Kinect was used to develop a training system that implemented a NUI application using Kinect to extract the variations of parts (elbow, shoulder, etc.) from the whole body by capturing the whole body at the time of CPR training to detect the whole-body input, and to make correct and incorrect judgments of the shape of CPR’s postures.
4. System Interface Overview
In the interface, we developed an analyzable system to visualize and analyze subjects’ training attitudes in AR (augmented reality) representation, and the processing which relied on the anatomical knowledge [5],[6] was carried out on Body Tracking detection data of Kinect. Therefore, this system can be used to determine the correct (or incorrect) position of CPR without wearable devices, which are required by motion capture etc.
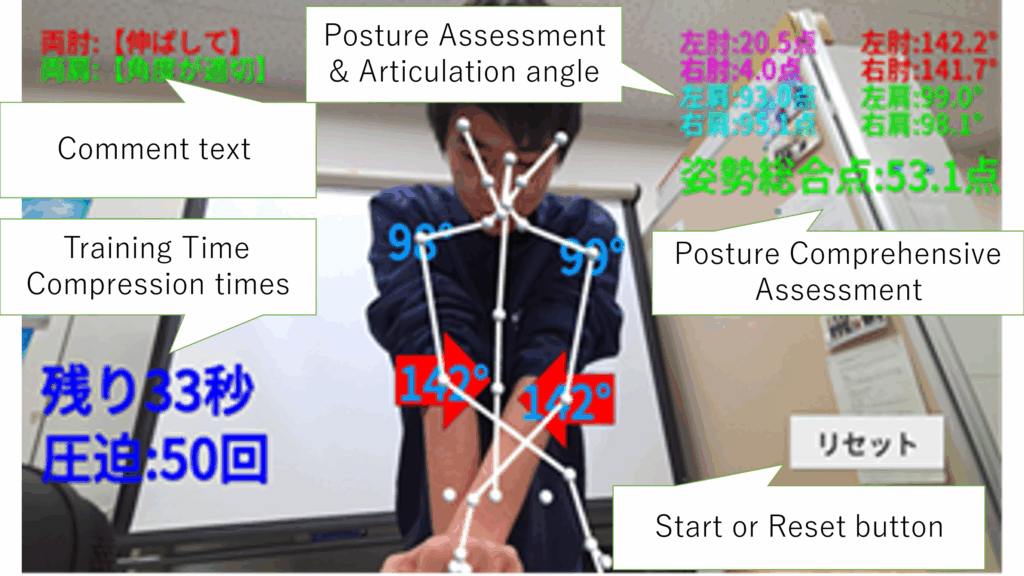
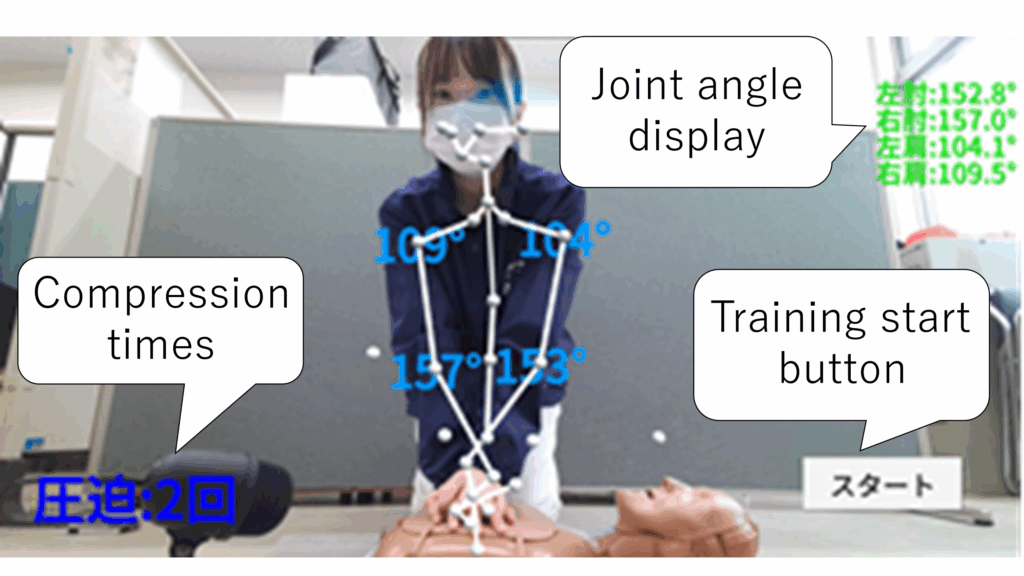
As shown in Figure 2, the frontal Kinect display interface derived detection and assessment of the left and right elbow and shoulder in real time and displayed a point transform (100-point method) to make it easier for trainees to recognize.
Comment labels are displayed according to the condition of each joint, and arrow marker interfaces point to incorrect postures and are displayed relative to where they should be corrected.
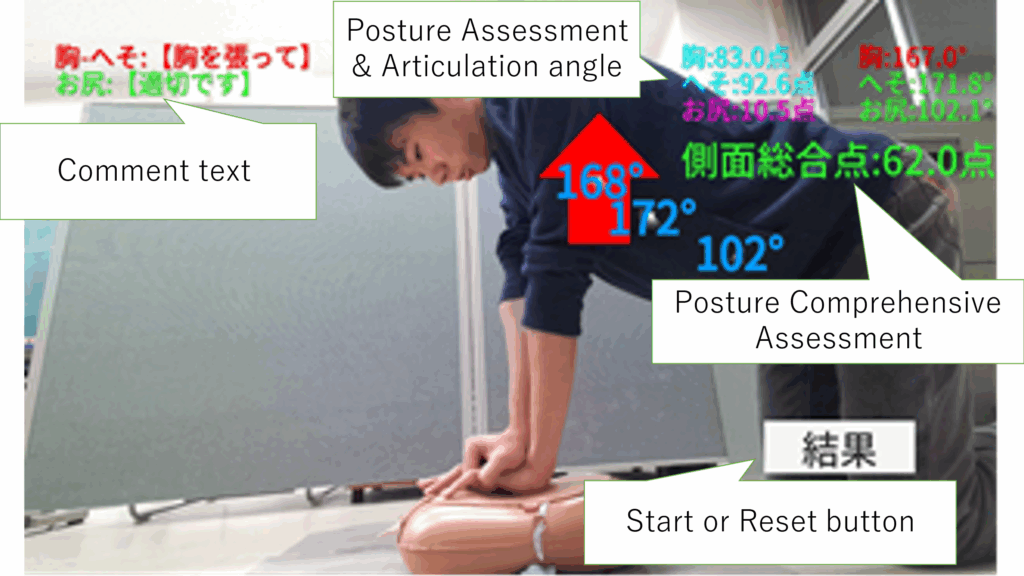
In the lateral Kinect display interface as in Figure 3, detection and assessment of the chest (thorax), navel (abdomen), and buttock were performed in real time to display the number of points and comments as well as the interface of arrow markers in the direction to be modified. These interfaces have been implemented as NUI applications using the game engines Unity.
5. Correlation Between the Coefficient Processing of the Number of Compressions and the Postural Total Point
As mentioned above, the counting process of the number of compressions implemented in this system detects a total of two clicker sounds during compression and decompression when a CPR training doll is compressed to an appropriate depth using a single-directed microphone, and counts the number of compressions. This clicker sound has a difference in sound pressure between when the sound pressure has reached an appropriate depth and when the sound pressure has not reached an appropriate depth. Using this difference, only an appropriate sound pressure (mean 77.9dB) is recognized as the number of compressions.
A positive correlation between the number of compressions and the postural score has been demonstrated in a previous study in a poor laboratory.
Training time is 1 min. A countdown of the remaining time of training is displayed at the bottom left of the screen. As for the number of times of compression, two clicker sounds (metallic sounds) generated when CPR training doll is compressed and decompressed to an appropriate depth (about 5 centimeters) are detected by a single directional microphone, and the number of times of compression is counted as one time by two clicker sounds.
6. Relationship Between Compression Posture and Hand Placement (Hand Shape)
The training features of NUI application developed in this study can capture the trainees’ own CPR postures and learn the correct CPR training while modifying their own postures. Conventional studies using this system have analyzed the position and angulation of the elbow, shoulder, lower back, and chest from the front and side using this feature, and have investigated the basic form (shape; kata) of the position to perform CPR. One of the key elements of CPR that has not been analyzed so far is how to place the hand (hand kata). Traditionally, there have been no evidence-based findings referring to the effect of CPR on the efficacy of hand kata, and it has not been elucidated what effect the hand kata has on CPR’s posturing.
On the other hand, when CPR training is practiced, trainees are carefully concerned about the hand part, and trainees have also been seen to change the placement and compilation method in the middle of training.
Therefore, the kata of the hand, which is considered to be a critical site when performing CPR training, was analyzed from two perspectives, namely, the postural total point from the training system (front and side) and the exercise load (increased pulse volume), on the effect of the upper and lower changes of the dominant hand, as shown in Figure 5. CPR has a high exercise load, and even a 1-min training using the system requires a substantial amount of exercise. It is said that it takes an average of 8 minutes for an ambulance to arrive at the scene when encountering a scene of cardiac arrest and performing critical care activities. Considering that laypersons perform CPR for more than 8-10 minutes before delivering a cardiac arrest treatment to the ambulance, it is crucial to reduce the exercise load more.
7. Experimental Methods and Overview
The experiments were conducted in February 2023 for the first experiment with 30 people (18-24 years old) and in May to June 2023 for the second experiment with 33 people (18-23 years old) in total for two times. The experimental methods are outlined in Figure 5 (the first experiment) and Table 1 (the second experiment) below.
7.1. Overview of the first experiment
In the first study, we analyzed whether there is a change in postural and exercise loads by changing the kata of the hand during CPR training.
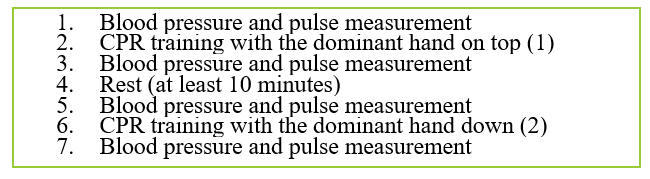
For Figure 5 ①, ③, ⑤, and ⑦, the increase and decrease of pulse was used as an index of exercise volume, so blood pressure and pulse were measured before and after CPR training. Pre-and post-training pulse rates were compared, and their increments were analyzed by determining differences between those with the dominant hand up and down to determine which exercise dose was more reduced. In ② and ⑥ of Figure 5, training using CPR training system was carried out, and postural total points were analyzed from the front and side in the training of ① and ② in which the dominant hand was changed. In Figure 5 ④, the pulse rate at rest was used as a reference, and a break of more than 10 minutes was set for the purpose of lowering the increase in the pulse by the training performed with the first handedness.

7.2. Outline of the Second Experiment
The effectiveness of the result on the positioning method of the hand in CPR which was proven by the first experiment was verified. The newly conducted experiment (the second experiment) for verification was conducted from May to June 2023 with 33 subjects (18-23 years old). In the second experiment, the body composition, back muscle strength, and grip strength of the subjects were newly measured in addition to the survey on the method of hand placement, and various factors were examined for analyzing CPR postures. The experimental methods and procedures performed in the second experiment are as shown in Table 1 below.
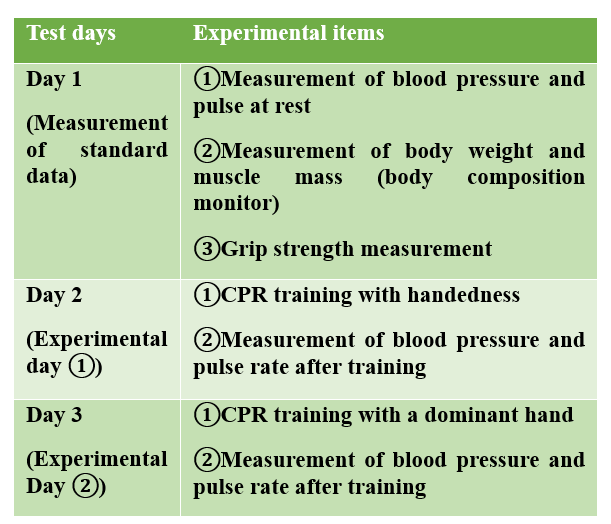
Table 1: Methods and Outline of the Second Experiment
 Measurements of physical data, such as blood pressure and pulse measurements, were performed under supervision by nurse-qualified medical personnel.As a cautionary note in measuring blood pressure and pulse, it was noticed that exercise and meal within 2 hours before measurement should be refrained, that the arm in the measurement is used in principle of the same person’s arm, and that the number rise due to tension similar to white coat hypertension in the measurement should be sufficiently considered.Changes from the first experiment and additional experimental items are described below.
Measurements of physical data, such as blood pressure and pulse measurements, were performed under supervision by nurse-qualified medical personnel.As a cautionary note in measuring blood pressure and pulse, it was noticed that exercise and meal within 2 hours before measurement should be refrained, that the arm in the measurement is used in principle of the same person’s arm, and that the number rise due to tension similar to white coat hypertension in the measurement should be sufficiently considered.Changes from the first experiment and additional experimental items are described below.
The first change in the experimental method was the experimental method in which the trainee changed the upper and lower of the dominant hand in the first experiment, experienced the training twice in a day, sandwiched a break between the training to handle the pulse, and returned the pulse to the normal value. In this regard, in the second experiment, by dividing the experiment into three days (experimental day ② performed after 1 week), such as various reference values measurement days (resting blood pressure and pulse, grip strength, and body composition data), experimental days ① (CPR training with the dominant hand down), and experimental days ② (CPR training with the dominant hand up), the pulse values at rest and after the training were acquired more precisely than those in the first experiment.
As the second change point of the experimental method, the case in which the dominant hand was put up was carried out first in the first experiment, therefore, in the second experiment, the training in which the dominant hand was put down was carried out first in the second experiment, and whether the change occurs in the experimental result of the first experiment by changing the order was verified, and the result in the first experiment was confirmed. As a change point of the third point of the experimental method, the dominant hand was investigated by the questionnaire in the first experiment, and the chapman test was used for the discrimination of the dominant hand in the second experiment.
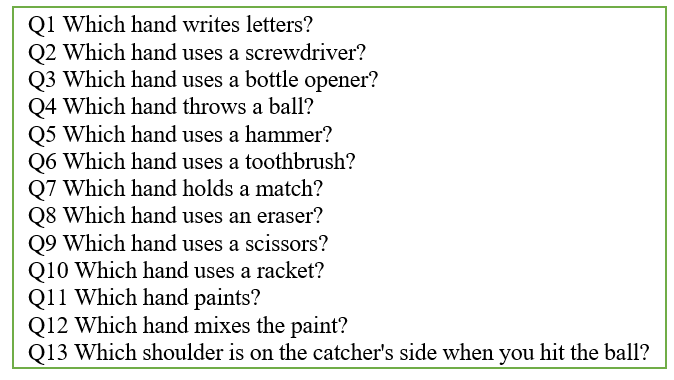
The chapman test is a test of the method which chooses and answers the question of 13 items from 3 choices of right hand, both hands and left hand. It is converted to 1 point in the right hand, 2 points in the both hands, 3 points in the left hand, and the discrimination of the dominant hand is carried out by the total point in all 13 items. The questions of the Chapman test actually used in the experiment are as described in Figure 7 below. The calculation method of the total score is right-handed 13~17 points, both-handed 18~32 points, and left-handed 33~39 points.
In the second experiment, a total of 11 items (14 items) including grip strength, back muscle strength, muscle mass (both arms, both legs, and trunk), body fat percentage, height, weight, difference in centroid position according to gender, sitting height, opening knee, positional relationship of the site after the knee, and head position were measured and observed before the experiment.The second experiment was conducted with the above changes and new experimental items added.

8. Results of the First Experiment
The developed CPR training system is capable of objectively assessing correct postures during CPR. In the first experiment, in order to investigate the correct posture in chest compressions, the authors noticed the kata of the hand to perform compressions. In this study, we comparatively analyzed the changes in postural assessment points, number of compressions, and exercise loads in CPR training system to determine the effects of hand kata on CPR in the correct posture, and derived statistical outcomes from each relation. Table 2 shows the results of the first experiment with 30 subjects.
The mean was calculated for each postural total score in the frontal and lateral systems and for the increase and decrease of the pulse before and after training, and the significance probability was determined by Wilcoxon signed rank test for the difference between the means.
Table 2: Experimental Results of the First Experiment
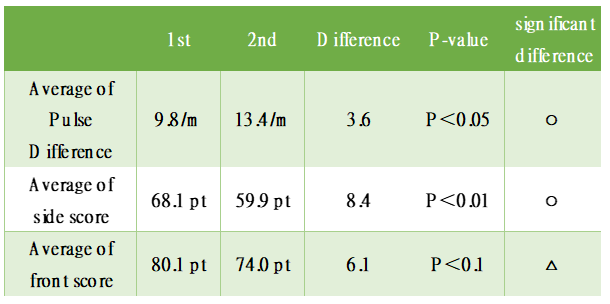
As shown in Table 2, there were significant differences in the means of CPR training between the first (training with the dominant hand up) and the second (training with the dominant hand down) in the two items of the pulse and the postural total points of the lateral system. And, the result that it showed the significance tendency was obtained, though the significance could not be confirmed on posture total point of the frontal system. As shown in Table 2, there was an average difference of 3.6 movements for the pulse, an average difference of 8.2 points for the lateral posture total point, and an average difference of 6.1 points for the frontal posture total point.
These findings demonstrate that a good CPR can be performed when the dominant hand is placed above, compared with when the dominant hand is placed below. This finding suggests that the dominant hand must be raised as a CPR hand kata as an early experiment to elucidate the optimal kata of CPR.
9. New Challenges from the Results of The First Experiment
Though the result obtained in the first experiment was good, it is necessary to reexamine the effect of the order of the training on various items and the effect on blood pressure and pulse [7], because the training for the dominant hand is carried out before and the training for the dominant hand is changed under, and because the training was carried out twice in the same day. As items that need to be verified, it is necessary to confirm that a significant difference in postural score and pulse could have been generated by the experimental method of performing training when the dominant hand is advanced, followed by training when the dominant hand is changed to the lower hand.
As for the postural total point, the exercise load by the training is large, so if the training is carried out during the same day, the fatigue by the first training, etc. seems to have an effect on the second training. On the other hand, for the second training, since the trainee is also experiencing the training once, it is possible that the trainee learns and corrects the posture, and therefore there is a possibility that the total posture point on the front side tends to increase more easily than the first training. Blood pressure and pulse were also performed after the first training until the pulse was lowered to the same level as normal, but because the first training and the second training were performed on the same day, it was speculated that fatigue might be influenced during the second training.
To obtain more accurate data, it was necessary to test the results of the first experiment by changing the training sequence and taking measures such as taking each training on different days.
10. Results of the Second Experiment
The results revealed by the second experiment, which was conducted as the development of the first experiment, are described below. One of the objectives of the second experiment is the verification of the experimental results that “the dominant hand should be put up” on the proper hand placement obtained by the first experiment. Detailed figures are summarized in Table 3. In conclusion, the results of the second experiment were similar to those of the first experiment. Wilcoxon’s signed rank test was performed on the total postural total points (frontal and lateral) and the amount of motion (increase in pulse) obtained in the experiment for a total of two training sessions in which the upper and lower dominant hands were changed, revealing a significant difference in the difference between means.
This result verified the result that “the dominant hand should be placed in CPR position” obtained in the first test. Table 3 shows the results of the second experiment. In the first experiment, we compared the postural total points of the pulse and the lateral system, which were found to be significantly different. The first CPR training was performed with the dominant hand down and the second CPR training with the dominant hand up. The test method is Wilcoxon signed rank test.
Table 3: Results of the Second Experiment
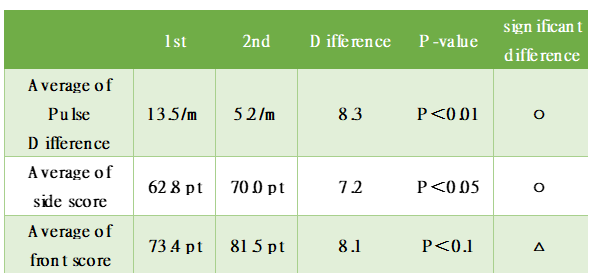
The mean increase/decrease in pulse was 13.5 for the first training and 5.2 for the second training. The difference in each mean was 8.3 times, and the significance probability for this difference was found to be significant because the P value was 0.00061 and P<0.01.
The average of posture total point in the side system became 62.8 points in the first time average and 70.0 points in the second time average, and the difference became 7.2 points. The probability of significance for this difference was found to be significantly different from P<0.05, with a P value of 0.045.
In the first experiment, the average of postural total points in the frontal system which showed an extremely high significance tendency was 73.4 points in the first time, and 81.5 points in the second time, and the difference became 8.1 points. For this difference, the significance probability became P value of 0.1, so no significant difference could be identified, but it showed a significant trend.
In addition, the results of the Chapman test performed in the second experiment showed that 26 of 33 trainees (78.8%) fell into right-handedness, 7 (21.1%) fell into left-handedness, and 0 were double-handers.
The following hypothesis was obtained as an observation result of two experiments carried out in this study:
In the first, it became clear that it was important to place the dominant hand as a kata of CPR’s hand “above”, but it was considered that there might be a difference according to the mastery level. For inexperienced persons and trainees whose CPR had difficulty, the hand (particularly the wrist) was painful or the force transmission was unstable when the dominant hand was placed on the top, because the force (muscle force) of only the dominant hand was to be applied. Based on these observations, we believe that it is important to grasp the base of the palm of the upper hand so that it is touched on the back of the lower hand as a grasping method for making the dominant hand up.
Second, there is a problem with the need to keep the fingers of the lower hand in close contact. It appeared that the lower hand’s palmar base could be focused on the sternum, and compressed at a single point without dispersing the force, by allowing the fingers of the lower hand to be floated by the hand grasping from above, rather than by placing the entire hand on chest compressions. However, this finding is also influenced by sex differences and individuality of muscle mass and body weight, so further analysis will be advanced in the future.
Third, the normality of the frontal total point and the number of compressions was confirmed for the values derived by this system. However, because of the problem of the number of experimental samples in this study and the necessity of examining the effects of sex differences, nonparametric methods were used in the present experiment.
11. New Findings from the Second Experiment
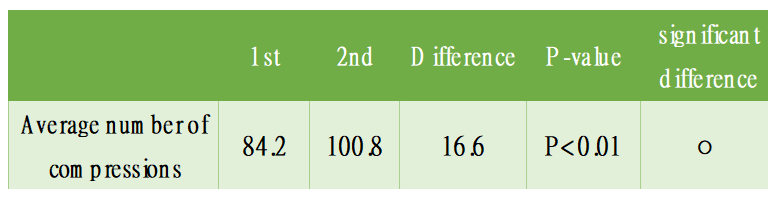
As a result of the new analysis and examination in the second experiment, it was newly proven that the effect of up and down of the dominant hand on the number of compressions, the change of up and down of the dominant hand during chest compressions had an effect on the quality of compressions (appropriate depth and position). As shown in Table 4, the mean number of compressions counted on the system differed by 16.6 in the first and second training sessions, and the results of the tests showed that the differences were significant.
The results reveal the importance of superior handedness in terms of providing adequate compression.
Table 4: Difference in Mean Number of Compressions and Test Results
12. Correlations Between Muscle Strength and Muscle Mass of Body Components and CPR
As an item newly analyzed in the second experiment, there is the effect of muscle force and muscle quantity which are the component of the body on CPR. The muscle force analyzed in this study is 3 items of back muscle force and left and right-hand grip strength, and the muscle quantity is 4 items of left and right arm, whole-body and trunk division.
As a result of the analysis of the second experiment, it was proven that there was a positive correlation between muscle force and muscle quantity and compression frequency only when the dominant hand was raised. The correlations were high in three items: back muscle strength (correlation coefficient: 0.497), left handgrip strength (0.559), and right handgrip strength (0.452), whose correlation coefficients ranged from 0.4 to 0.7. Four items, including total body muscle mass (0.339), trunk muscle mass (0.338), right arm muscle mass (0.315), and left arm muscle mass (0.269), corresponded to correlation coefficients between 0.2 and 0.4, which were considered to be somewhat correlated.
From this finding, it was clarified that the handedness was important in order to utilize muscle force and muscle quantity in CPR. In addition, as new observations, trainees whose muscle strength and muscle mass did not reach a certain standard were unable to compress to an appropriate depth during compression, and they were found to have a scene in which the clicker sound did not sound. In the future, we will conduct experiments focusing on the values of muscle strength and muscle mass, and aim to elucidate the minimum necessary muscle strength and muscle mass for performing CPR.

13. Challenges in the Second Experiment
In the second experiment, the results of the experiment proved that the dominant hand had to be placed on the top, which was found in the first experiment. On the other hand, for katas in other parts of the hands other than kata, in the second experiment, it remained in the observation record of the posture and the stage of data measurement.
In the future, based on the results of the second experiment, after extracting the items to be newly elucidated, the experiment will be conducted according to the extracted items. The items to be tested in future experiments are the positional relation of the knee on the ground in CPR posture and the effect of the position of the head on CPR posture.
14. Threshold-Derived Joint Angles of CPR Training Systems
In CPR training system which analyzes CPR posture, the objective evaluation is carried out on the basis of the value of the joint angle during the training, when the posture total point is derived. For the purpose of elucidating the more precise numerical value of this joint angle, the third experiment was carried out for 68 persons (18-21-year-old) in July, 2023.
15. Third Experiment: Analysis of Joint Angles
In the third experiment, which aimed to analyze the joint angles of CPR, the number of samples acquired is approximately 3500 compressions. For each compression detection, the joint angles of the upper and lower extremities were recorded in the system, and a total of seven joint angles were statistically analyzed to derive a threshold of appropriate joint angles during compression. Angle thresholds take into account the points implemented in the system and use interquartile ranges.
We judged it reasonable to use an interquartile range, which is the median 50% of the data, as the reasons for using the interquartile range are all normality of the joint angle data, and the use of a range of minimum to maximum values as a threshold is dangerous to include outliers.
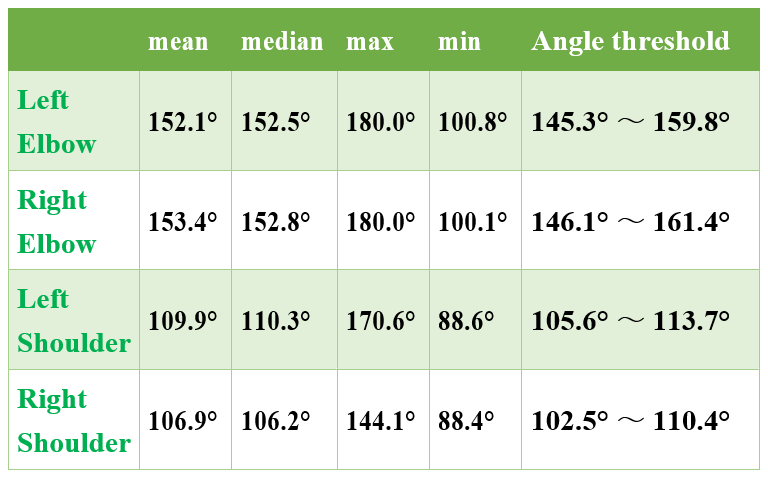
There was a total of 4 observation points of elbow (left/right) and shoulder (left/right) for the joint angle of the upper extremity, and the results of each analysis (mean, median, maximum, and minimum) and the interquartile range (angle threshold) were shown in Table 5 below.
Table 5: Analytical Results of Upper Limb Angle
Regarding the joint angle of the lower extremities, the results of each analysis were as shown in Table 6, according to three observation points in total: chest, navel, and buttock. From the result of this experiment, the range of joint angle which can be called appropriate chest compression posture was proven. In addition, all the data obtained in the experiment had normality.
Table 6: Analytical Results of Leg Angle

16. Results of the Third Experiment
Experiments performed in this study revealed angles of individual joints in CPR postures. Though chest compressions were traditionally the weather of compressing the heart, the analysis of trainee compression in this experiment revealed the distribution of joint angles when performing appropriate compressions, and there was a discovery that the interquartile range of the angles was converged within 15 degrees for all joints.
Since previous studies have revealed correlations between muscle mass and muscle, this study has demonstrated that posture and muscle mass and strength are components that affect CPR. In the future, it is considered that this test will be a great step in the review of conventional posture score (assessment) derivation algorithms in the elucidation of the appropriate posture of CPR.
17. Appropriate Joint Angle and Systematic Implementation of CPR Postures
Implementation of the system using joint angle thresholds derived by this study was completed in August 2023.
In addition, CPR training system will be a new stage, and CPR training system will be further upgraded by conducting experiments with healthcare professionals such as paramedics and nurses who are professional professionals in critical care settings.

As of September 2023, we have been conducting experiments and posture analysis with the cooperation of professionals such as paramedics, nurses, assistant nurses, and mobility rescuers, with a total of approximately 30 members from the JSDF, the Maritime Guard Agency (Japan Coast Guard), and the Kushiro City Fire Department.

By analyzing the attitudes of professionals, we believe that it will be possible to advance CPR training system that has been developed for lay people to a professional system that can also be used by people in life-saving settings.

To continue the analytical study of CPR postures based on joint angles, and to seek the introduction of artificial intelligence (AI) as the development of this system in the future. In the assumption at present, it aims at the establishment of the new posture evaluation method using the neural network.
18. Development of an AI System for CPR Posture Evaluation
This research, which clarified the effects of partial posture changes on compression and analyzed posture as a clear numerical value of joint angle, realized the development of a new system to derive CPR posture evaluation by AI technology (neural network) as a new stage. The AI system for CPR posture evaluation was developed for the purpose of analysis considering the connectivity of the human body and the individuality of the trainee, which has been a problem in the posture evaluation of conventional CPR training systems. The data learned in implementing these posture evaluations are the training data of 101 trainees and approximately 4,700 training sessions accumulated in the experiments conducted in this study. The training data refers to the joint angle values during compression detected by voice recognition during training using the CPR training system. It was found that the training data for each joint had normal differences. The trainees consisted of 68 general public and 33 lifesaving professionals (medical and emergency scene workers).
As shown in Figure 14, the numerical values of each joint angle obtained during training using the CPR training system when the appropriate pressure is detected by voice are processed for posture evaluation by the AI. The CPR training system and the CPR posture evaluation AI system are connected by a socket to enable prompt provision of feedback after training.
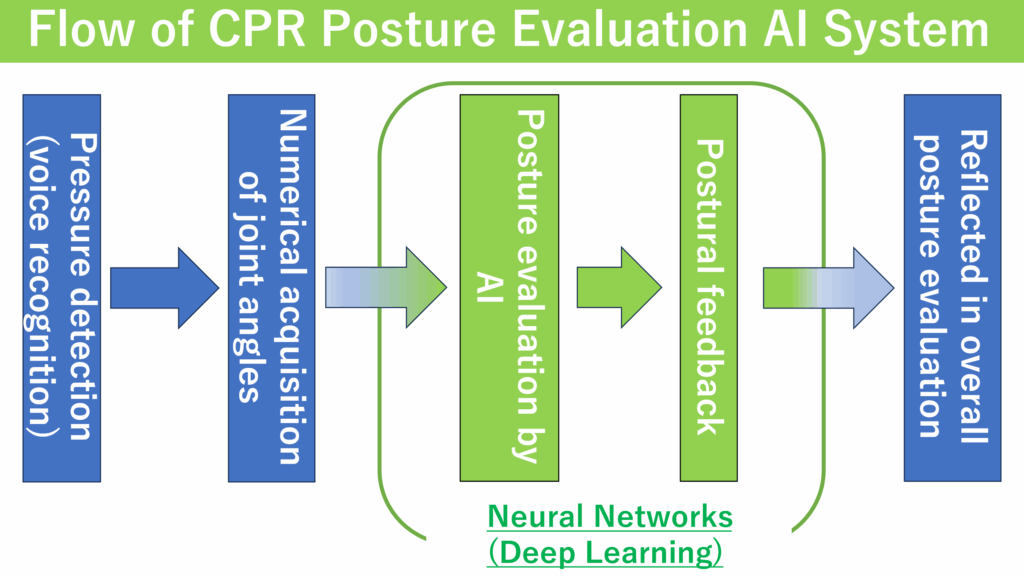
19. Feedback on Posture
In the CPR training system, the evaluation was derived based on the numerical values of joint angles and referred to the preset threshold values. On the other hand, in the new system, which is a multi-layer learning system with neural networks, it provides feedback (postural feedback) on the characteristics of the trainee’s CPR posture and weaknesses and vulnerabilities during CPR.
20. Conclusion
In this study, attention was paid to the hand performing chest compressions as an early study to elucidate the proper posture (shape; kata) of CPR, and the effect of the change of the upper and lower handedness on the whole CPR posture was elucidated from the values such as postural total point of the training system, exercise load (increase of pulse), and the number of compressions. In conclusion, the results of the experiment revealed that placing the dominant hand on top resulted in excellent results for both postural composite point and exercise load. It is also considered that there were great achievements in terms of clarifying the correlations between CPR and muscle strength and muscle mass, and extracting the components that seem to affect CPR. And, the precise numerical value of the joint angle of CPR position was analyzed by the third test, and it seems to become a big step for the elucidation of the kata of the appropriate CPR as well as stepping up the future CPR training system research to the next stage.
By demonstrating previously unexplained joint angles in CPR postures on a scientific basis, we are convinced that training can be established that allows the implementation of continuous CPR over a prolonged period of time without the use of wasteful forces by compressing them in an appropriate posture, even in the presence of body disparities. In the next stage of the study, the posture in CPR is extracted using the parts constituting the posture as elements, and how each part brings about the change in CPR posture and compression frequency, and what kind of catastrophe exists for each part in order to reduce the motion quantity are elucidated. Further experiments will elucidate not only the effects of one site, but also the effects of a particular site on adjacent sites, and the effects of a particular site on overall posture.
This study is a steady study to elucidate the unknown attitude of life saving methods related to the forefront of human life saving called CPR.
We hope that this study will be a step-in saving people who have suffered a cardiac arrest, and we will definitely clarify the appropriate attitudes of CPR. Cardiac arrest is a constant risk-of-being, while CPR may be able to control it.
This study will be developed in the future so that more human life can be saved by the elucidation of the appropriate CPR attitude.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgement
This is a related study on the topic “Elucidation of the optimal postural and movement of chest compressions in CPR” adopted in the 2024 Basic Research (C) Kaken Cost Task Number 23K11336 in the Scientific Research Grant Project of the Japanese Society for the Promotion of Science. We thank the public and others for its affiliation.
We thank mobility rescuers at the Kushiro Air Base of the First District of the Maritime Safety Agency who have cooperated in the experiments, sailors of the Japan Marine Self-Defense Force, the Japan Ground Self-Defense Force, and the Affiliated Department of the Central Fire Department of Kushiro City Fire Department.
In addition, I would like to thank Mr. Yukiko Yoshida, a nurse of the Kushiro Public University Health Room who supervised the measurement of various physical data during the second experiment, Mr. Miyuki Yasuda, Mr. Tomoki Kuriyagawa, Mr. Yuki Senno, and other members of the monthly laboratory who gave great advice on this study.

- Taiki Yamakami, “Study on the Effectiveness of Training Using CPR Form Teaching System”, 2023.
- Tomoki Kuriyagawa , “Developing and Evaluating CPR Training Systems”, 2021.
- Editorial Board to JRC Resuscitation Guideline 2020 “JRC Resuscitation Guideline 2020”, 2021.
- Microsoft, “Azure Kinect DK Documentation”, The link was confirmed in June 2023, https://learn.microsoft.com/ja-jp/azure/Kinect-dk/
- Masato Tutiya,” Mutual knitting of this shoulder, which reveals the “why” of the attitude and movement useful for guidance on sports and health development”, 2018.
- Institute for Medical Informatics,” First Edition of Physical Assessment”, 2015.
- MHLW Japan, “Blood pressure | Health events & content”, Linked June 2023, https://www.smartlife.mhlw.go.jp/event/disease/pressure/
No. of Downloads Per Month