Effect of Knee Orthosis on Lateral Thrust in Patients with Knee Osteoarthritis
Volume 7, Issue 5, Page No 41-45, 2022
Author’s Name: Hiroaki Yamamoto1,2,a), Masahide Endo3, Tomohiro Baba3, Chikamune Wada2
View Affiliations
1Department of Physical Therapy and Fukuoka Tenjin Medical Rehabilitation Academy, Fukuoka, 8100004, Japan
2Graduate School of Life Science and System Engineering, Kyushu Institute of Technology, Kitakyushu, 8080196, Japan
3Sakurajyuji Fukuoka Hospital, Fukuoka, 8100004, Japan
a)whom correspondence should be addressed. E-mail: h.yamamoto.28.0321@gmail.com
Adv. Sci. Technol. Eng. Syst. J. 7(5), 41-45 (2022); ![]() DOI: 10.25046/aj070506
DOI: 10.25046/aj070506
Keywords: Lateral Thrust, Knee Orthosis, Wearing Pressure, Knee Osteoarthritis

Export Citations
To examine the effects of wearing a flexible knee orthosis (FKO) on the lateral thrust in patients with knee osteoarthritis (OA) by changing the wearing pressure. This study was a cross-sectional study. Thirteen patients (mean age: 82.8 ± 7.5years with Kellgren Lawrence Stages I and II knee OA were included and prescribed FKO. Patient with osteoarthritis of the knee was attending outpatient rehabilitation. Using a wireless 3-axis accelerometer, we analyzed the lateral thrust in the proximal lower leg during walking (10 m) with the knee orthosis under different wearing pressures (without orthosis, using “standard force” of application, and using “tight force”). The peak values in the outward direction of the gait cycle over the three experimental conditions were selected for analysis. The mean values for patients with K-L stages I and II were calculated and compared. We found that “tight force,” i.e., tightening the hook-and-loop fastener of the knee orthosis to its maximum, resulted in significantly lower lateral thrust compared to the absence of an orthosis. The effect was more pronounced in K-L Stage II patients. Our findings confirm that increasing the wearing pressure of the knee orthosis reduces lateral thrust in patients with knee OA. In Stage 1, the lateral thrust could be suppressed by the “standard force,” but the lateral thrust in “Stage 2” required “tight force” to be suppressed. Knee orthosis for knee osteoarthritis were found to have the potential to inhibit lateral thrust.
Received: 1 August 2022, Accepted: 05 September 2022, Published Online: 14 September 2022
1. Introduction
Knee osteoarthritis (OA) is a degenerative disease of the knee joint that affects the joint tissues, such as articular cartilage, meniscus, and ligaments [1-3]. Once the joint degeneration commences, 30% of the healthy knee joint structures will be affected within two years, while 90% of joints is affected within the next 11 years [4].
Based on the compartment affected, the disease is classified into medial, lateral, patellar, and total variety [5]. In the Japanese population, 90% of all OA patients have medial compartment OA with an internal deformity [6], which involves impairment of the periarticular ligaments and other supporting tissues, resulting in a lateral sway of the joint. Consequently, a lateral thrust is observed during walking as the outside of the knee is pushed laterally (Figure 1) [7, 8].
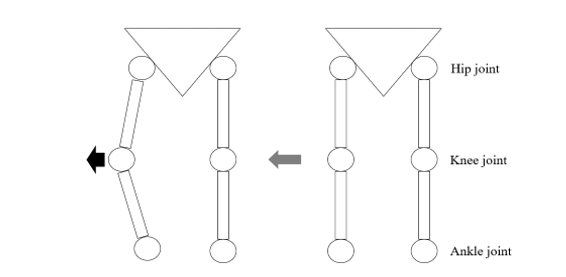
Figure 1: Schematic diagram of lateral thrust in an osteoarthritic knee during walking
The mechanical stress of repeated postures and movements in daily life is a crucial factor triggering disease onset [9]. Accordingly, a flexible knee orthosis (FKO) made of elastic materials is often used to counter these mechanical stresses. The FKO comes in a wide range of shapes, including those with bands and struts for alignment and knee stabilization. While flexible orthosis is not as supportive and does not provide as much corrective force as rigid knee orthosis, it is widely used by OA patients because it is inexpensive, lightweight, and easy to install [10].
It has been reported that wearing FKO reduces the knee varus moment, suggesting its role in suppressing lateral thrust [11]. Additionally, the FKO covers the entire knee, compressing and stimulating the periarticularis muscles of the knee joint. Therefore, the effect of external pressure tightness may be responsible for restricting abnormal motion and reducing the pain.
Previous studies have shown that wearing FKO suppresses the lateral thrust [11]. However, the effects of a change in wearing pressure have not been elucidated. There is evidence to support that muscle activity is improved by increasing the wearing pressure of the orthosis [12]. Therefore, the pressure exerted by the orthosis may affect muscle activity to correct deformity and lower limb alignment, thereby improving knee stability and controlling abnormal motion. The orthosis can limit abnormal motion in the initial disease to reduce pain and support stability. Accordingly, by increasing the wearing pressure of FKO, the knee joint may become relatively fixed, restricting abnormal movements and leading to pain.
Therefore, the current study investigated whether FKO with different wearing pressures can affect the lateral thrust in patients with knee OA.
2. Materials and methods
2.1 Research Participants
We included 13 patients with knee OA. The severity of knee OA was determined using the radiological Kellgren Lawrence (K-L) classification index [13], according to which, nine patients belonged to Stage I and four patients had a Stage II disease with mild varus deformity. Patients who had hip and ankle other orthopedic diseases and symptoms, or those who had resting pain or tumor in the acute phase. were excluded from the study. This is because those symptoms could affect gait. Controls and interventions were provided to all13 patients. The study was conducted as per the Declaration of Helsinki and was approved by the Research Ethics Committee of the Sakura Juji Fukuoka Hospital, Japan (Approval ID: 2021070501). The purpose and methods of the study were explained to the research participants. Consent to participate in the study was obtained in writing.
2.2 Measurements
To measure the lateral thrust, a wireless 3-axis accelerometer (Q’s TAG; Sumitomo Electric Industries, Ltd., Konohana-ku, Japan.) was used. The device allowed for measuring the knee joint external deflection angle during walking without affecting the patient’s gait since the accelerometer is small and lightweight (41 × 41 × 14.5 mm3 and 15 g, respectively). The accelerometer was fixed to the fibular head (less affected by soft tissue-related artifacts) of the affected limb using Velcro in a standing position (Figure 2). At a sampling frequency of 200 Hz, the acquired data were wirelessly fed into a personal computer via Bluetooth. Patients were asked to walk for 10 m at a comfortable pace. Using Ogata’s method [14], a sudden acceleration change in the outward direction at the beginning of the stance was defined as lateral thrust; accordingly, the peak value of outward direction of the during walking was used for analysis.

Figure 2: Placement of the accelerometer on the fibular head of the affected limb
An open-type FKO (Facilitated Supporter: (Nippon Sigma Max Co, Ltd., Shinjuku-ku, Japan) was given to all patients (Figure 3). The orthosis size was indexed by the length around the thigh–0.1 m above the center of the patella. A numerical size close to the median of the orthosis was used. The following three experimental conditions were implemented: (1) the participant did not wear the orthosis (hereafter, “control”), (2) the orthosis was fastened with appropriate force (“standard force” condition), and (3) the orthosis was fastened with a fully tightened hook-and-loop fastener (“tight force” condition). The appropriate force meant the force applied to achieve a comfortable and firm fit. All fittings were undertaken by a single physical therapist. All measurements were performed once for each research participants (Figure 4).

Figure 3: Flexible knee orthosis
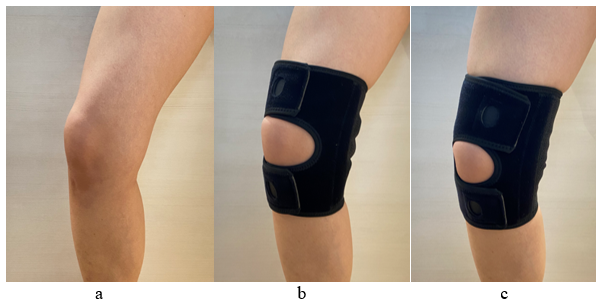
Figure 4: Different wearing pressures of the orthosis.
a: the participant did not wear the orthosis
b: the orthosis was fastened with appropriate force
c: the orthosis was fastened with a fully tightened hook-and-loop fastener
The wearing pressure of the orthotics was measured using an airbag-type pressure sensor “Palm Q” (manufactured by Cape, Ltd., Osaka, Japan). According to Laplace’s law [15], the wearing pressure exerted on the lower limb is directly proportional to the tension generated from the orthotics applied to the curved surface of the lower limb. The center of the pressure sensor (10 cm2) was set to be 5 cm above the center of the patella, and the orthosis was attached on the sensor (Figure 5).

Figure 5: Palm Q sticking position.
The heel contact period was identified through vertical impact acceleration; one gait cycle was analyzed for statistical analysis (Figure 6, 7). The peak values in the outward direction of the gait cycle over the three experimental conditions were selected for analysis. Comparisons among the three experimental conditions were performed using the Friedman test and Tukey’s method. The JSTAT for Windows was used as the statistical software, and the significance level was set to 5%. The mean values for patients with K-L stages I and II were calculated and compared.

Figure 6: Measuring scenery
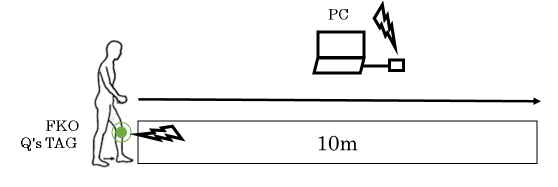
Figure 7: Schematic diagram of measuring scenery
3. Results
We included 13 patients with knee OA (6 males and 7 females) with a mean age of 82.8 ± 7.5 years (height: 156.0 ± 11.8 cm, weight: 53.2 ± 11.0 kg, and body mass index: 21.7 ± 2.3 kg/m2).
The wearing pressures were 14.3 mmHg, 41.2 mmHg for the Standard force, Tight force, respectively (Figure 8).
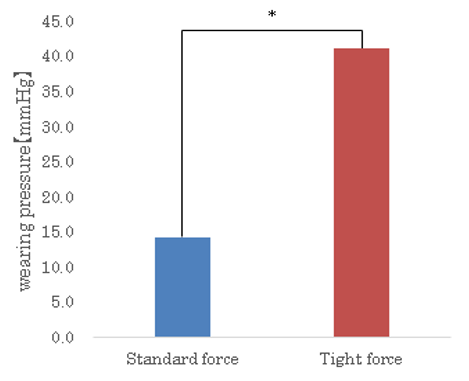
Figure 8: Comparison of wearing pressure
Conducted to quantify wearing pressure. All fittings were undertaken by a single physical therapist.
Table 1 shows the experimental results. Accordingly, our findings showed that the tight pressure condition promoted a significantly lower lateral thrust was significantly compared to the not wearing condition. Moreover, the lateral thrust was reduced by wearing a knee orthosis, and the lateral thrust tended to be further suppressed by increasing the wearing pressure (Table.1).
The mean values for lateral thrust detected in patients with Stages I and II OA are shown in Tables 2 and 3, respectively. Without the knee orthosis, lateral thrust was 15.3 m/s2, but with the knee orthosis, it decreased to 11.6 m/s2 in Stage I and 11.7 m/s2 in Stage II. In Stage I patients, the lateral thrust tended to decrease when the patient wore the orthosis (Table 2). Regarding the wearing pressure, there was no difference between different wearing pressures.
In Stage II patients, the lateral thrust was suppressed in the “tight force” condition compared to the “control” and “standard force” conditions (Table 3). Without the knee orthosis, lateral thrust was 17.2 m/s2, but with the knee orthosis, it decreased to 16.6 m/s2 in Stage I and 13.5 m/s2 in Stage II. Additionally, we observed that the more severe the disease, the more the lateral thrust, which was true for all conditions. In Stage 1, the lateral thrust could be suppressed by the “standard force,” but the lateral thrust in “Stage 2” required “tight force” to be suppressed.
Table. 1. Results of lateral thrust measured in patients with Stage I and Ⅱ osteoarthritis.
all values are mean ± standard deviation; units: m/s2
*:p<0.05(vs Control)
Table 2. Results of lateral thrust measured in patients with Stage I osteoarthritis.
all values are mean ± standard deviation; units: m/s2
Table 3. Results of lateral thrust measured in patients with Stage II osteoarthritis
all values are mean ± standard deviation; units: m/s2
4. Discussion
We found that the overall lateral thrust was reduced by using knee orthosis and was further reduced when the wearing pressure was increased. Furthermore, there was a significant difference between the “Tight force” condition as compared to the “Control” condition.
This reduction in lateral thrust during walking while donning FKO can be attributed to the improved fixation of the knee joint as well as the suppression of abnormal joint movement. Orthoses compensate for joint instability and abnormal movements caused by degenerated or damaged joint structures by providing external support to the joint [16]. The underlying objective is to reproduce the physiological movement of the joint as much as possible and prevent further damage to the joint structure [16]. Therefore, wearing a knee orthosis suppresses the lateral thrust to reduce the abnormal loading of the medial joint surface in the knee and the resultant pain and prevent disease progression [17].
Additionally, we observed that increasing the wearing pressure tends to suppress lateral propulsion which is probably influenced by the output of muscles around the knee joint. In a previous study, pressure stimulation changed rectus femoris muscle activity and knee angle improved jumping movements [18, 19]. Likewise, a study comparing muscle strength when wearing knee orthosis at different wearing pressures reported that with increments in the wearing pressure, the muscle output of the knee joint muscles increased and played an auxiliary role [20]. This is thought to be due to the fact that effective pressure stimulation is involved in suppressing muscle tone and promoting muscle flexibility [21]. A possible explanation is that the strongly stretched orthotic device works as an adjunct to the extensor muscle of the knee joint, i.e., the quadriceps [22]. Therefore, compared to the “standard force” condition, the “tight force” condition can better promote restrained abnormal movements, besides fixation of joint, which was also observed in our study.
There were certain limitations to the study results. The joint angle and muscle output were not measured; for this purpose, we plan to simultaneously measure knee joint movement and muscle power using a three-dimensional motion capture system and electromyography to correlate the effects of joint angle and muscle activity. Also, the patients were patients with mild knee OA (K-L Stages I and II); accordingly, differences in the severity of knee OA and internal and external deformities could not be localized. In Stage I patients, wearing the orthosis tended to suppress the lateral thrust but the effect of wearing pressure was very small. Likewise, in Stage II patients, the wearing pressure of the “standard force” condition was insufficient to suppress the lateral thrust, and a “tight force” may be necessary. These findings support the concept that the greater the disease severity, the more lateral thrust, and that the patients of stages I and Stage II show different trends. In recent years, it has been reported that pain emerges from early Stage 0 and Stage I knee OA, for which prevention has been emphasized, and some reports have defined Stage II and later as knee OA [23, 24]. Correspondingly, a greater lateral thrust was observed in Stage II than in Stage I. Therefore, it is conceivable that there is a need for stronger wearing pressure in Stage II. Accordingly, there is a need to increase the wearing pressure for knee OA patients based on their disease severity. The highest compression pressure a patient can tolerate is a maximum of 60 mmHg [25]. Compression stimulation of 30-50 mmHg decreases muscle stiffness and promotes flexibility [21]. Furthermore, regarding cell activation, it has been reported that the application of 30-40 mmHg of compression causes cell phosphorylation and promotes capillary dilation [26]. Therefore, the wearing pressure should be set at about 40 mmHg. However, the generalizability of our results is limited because of the small number of patients included. Future studies must include patients with varying degrees of disease severity.
5. Conclusion
The current study analyzed the lateral thrust in patients with knee OA during walking using FKO with different wearing pressures. We found that increased wearing pressure reduced the lateral thrust during walking, more so in patients with K-L Stage II OA. However, this study is limited in referring to the severity of knee osteoarthritis and the differences in internal and external deformities because they were not localized. For further research, we plan to simultaneously measure knee joint movement and muscle power to elucidate the reasons for lateral thrust reduction.
Conflict of Interest
The authors declare no conflict of interest.
Abbreviations
osteoarthritis (OA), flexible knee orthosis (FKO)
- W. Zhang, R.W. Moskowitz, G. Nuki, S.Abramson, R.D. Altman, N. Arden, S.B. Zeinstra, K.D. Brandt, P. Croft, M. Doherty, et al., “OARSI recommendations for the management of hip and knee osteoarthritis: part 2 OARSI evidence-based, expert consensus guidelines” Osteoarthritis Cartilage, 16(2), 137–162, 2008, doi: 10.1016/j.joca.2007.12.013.
- L. Sharma, “Local factors in osteoarthritis” Current Opinion in Rheumatology, 13(5), 441–446, 2001, doi: 10.1097/00002281-200109000-00017.
- R.A. Sch–ultz, D.C. Miller, C.S. Kerr, L Micheli, “Mechanoreceptors in human cruciate ligaments. A histological study,” Journal of Bone Joint Surgery AM, 66(7), 1072–1076, 1984, PMID: 6207177.
- S. Ikeda, H. Tsumura, T. TorisuIkeda, “Age-related quadriceps-dominant muscle atrophy and incident radiographic knee osteoarthritis,” Journal of Orthopaedic Science, 10(2), 121–126, 2005, doi: 10.1007/s00776-004-0876-2.
- T. Koshino, “Etiology of osteoarthritis of the knee, classification and clinical findings” Rheumatism, 25, 191–203, 1985.
- T. Koshino, “Knee osteoarthritis, knee clinic manual, 5th ed.” Medical and Dental Publishing, Tokyo, 2001.
- S. Knecht, B. Vanwanseele, E. Stüssi, “A review on the mechanical quality of articular cartilage – implications for the diagnosis of osteoarthritis,” Clinical Biomechanics, 21(10), 999–1012, 2006, doi: 10.1016/j.clinbiomech.2006.07.001.
- A. Chang, K. Hayes, D. Dunlop, D. Hurwitz, J. Song, S. Cahue, R. Genge, L. Sharma, “Thrust during ambulation and the progression of knee osteoarthritis,” Arthritis and Rheumatism, 50(12), 3897–3903, 2004, doi: 10.1002/art.20657.
- A. Mahmoudian, J.H. van Dieen, S.M. Bruijn, I.A. Baert, G.S. Faber, F.P. Luyten, S.M. Verschueren, “Varus thrust in women with early medial knee osteoarthritis and its relation with the external knee adduction moment,” Clinical Biomechanics, 39, 109–114, 2016, doi: 10.1016/j.clinbiomech.2016.10.006.
- T. Okamoto, Y. Ishii, M. Deie “Efficacy and Challenges of Orthotic Therapy” joint surgery, 38, 57–63, 2019, doi: https://doi.org/10.18885/j00282.2019374740.
- T. Okamoto, M. Deie, R. Asaeda, M. Kawano, C. Terai, H. Watanabe, M. Ochi “Examination of orthotic therapy for knee osteoarthritis using gait analysis” Separate Volume Orthopedics, 1(67), 121–124, 2015, doi: org/10.15106/J04037.2015223650.
- H. Yamamoto, S. Okamatsu, K. Kitagawa, C. Wada, “Effect of knee orthosispressure variation on muscle activities during sit-to-stand motion in patients with knee osteoarthritis,” International Journal of Environmental Research and Public Health, 19(3), 1341–1351, 2022, doi:10.3390/ijerph19031341
- J.H. Kellgren, J.S. Lawrence, “Radiological assessment of osteoarthritis,” Annals of the Rheumatic Diseases, 16(4), 494–502, 1957, doi: 10.1136/ard.16.4.494.
- K. Ogata, “Pathophysiology and treatment of knee osteoarthritis from the viewpoint of lateral sway,” Orthopaedic Disaster Surgery, 38(1), 11–18, 1995.
- M. Hirai, “Clinical application of compression stockings,” Especially about elasticity/elongation hardness and Laplace’s law,” Veinology, 23(3), 239–245, 2012. doi.org/10.7134/phlebol.23.239
- E. Genda, “Biomechanics of knee orthosis,” Bulletin of the Japanese Society of Prosthetic and Orthotic Education, Research and Development, 24(1), 9–15, 2008.
- A. Chang, K. Hayes, D. Dunlop, D. Hurwitz, J. Song, S. Cahue, R. Genge, L. Sharma, “Thrust during ambulation and the progression of knee osteoarthritis,” Arthritis and Rheumatism, 50(12), 3897–3903, 2020, doi: 10.1002/art.20657.
- D.K. Ramsey, K. Briem, M.J. Axe, L.S. Mackler, “A mechanical theory for the effectiveness of bracing for medial compartment osteoarthritis of the knee,” Journal of Bone and Joint Surgery. American Volume, 89(11), 2398–2407, 2007, doi: 10.2106/JBJS.F.01136
- G. Hayata, T. Miyakawa, “Effect of a wearing overlap length change of the knee joint supporter during a stop-jump task,” Japanese Journal of Physical Fitness and Sports Medicine, 63(2), 279–285, 2014, doi: org/10.7600/jspfsm.63.279.
- G. Hayata, H. Oka, K. Miyagawa, “Effects of supporter and the taping on isokinetic torque of the knee joint,” University of the Pacific Rim Departmental Bulletin Paper, 6(27), 199–203, 2012, doi: /10.24767/00000348.
- N. Miura, K. Kurosawa, M. Hirose, T. Suzuki, “Inhibitory Effects of Pressure on Soleus Muscle Motor Neuron Excitability and Flow Volume in Healthy Adults,” physical therapy science, 26(6), 773–776, 2011, doi: org/10.1589/rika.26.773
- H. Takigami, “Lateral knee sway and clinical symptoms during walking in patients with knee osteoarthritis,” Yokohama Med, 49, 505–510, 1998.
- N. Ozeki, T. Muneta, T. Saito, I. Sekiya “Concept of early knee osteoarthritis,” Bone Joint Nerve, 6(3), 473–479, 2016.
- M. Ishijima, S. Hada, H. Kaneko, L. Liu, M. Kinoshlta, H. Arita, J. Shiozawa, Y. Anwarjan, T. Aoki, Y. Takazawa, H. Ikeda, Y. Okada, K. Kaneko, “Expectations and challenges for the research of the early stage knee osteoarthritis in terms of the Kellgren-Lawrence classification,” Bone Joint Nerve, 6(3), 533–541, 2016.
- International Society of Lymphology ” The diagnosis and treatment of peripheral lymphedema 2009 Concensus Document of the International Society of Lymphology,” Lymphology, 42, 51–60, 2009.
- JS Martin, Wesley CK, Cody TH, Anna, EM, Joshua JS, Christopher BM, Michael DG, Andreas K, David DP, Lee Z, Michael DR ” Impact of external pneumatic compression target inflation pressure on transcriptome-wide RNA expression in skeletal muscle,” Physiol Rep, 4, 13209, 2016, doi: 10.14814/phy2.13029.
No. of Downloads Per Month
No. of Downloads Per Country