
Actigraph Analysis of Elderly Dementia Patients During Phototherapy Using Non-Linear Analysis
Volume 5, Issue 2, Page No 757-761, 2020
Author’s Name: Fumiya Kinoshita1,a), Yuki Mukumoto1, Keiko Teranishi2, Hideaki Touyama1
View Affiliations
1 Department of Electrical and Computer Engineering, Faculty of Engineering, Toyama Prefectural University, Toyama 939-0398 Japan
2 School of Nursing, Kanazawa Medical University, 5-11-80 Kodatsuno, Kanazawa, Ishikawa, 920-0942, Japan
a)Author to whom correspondence should be addressed. E-mail: f.kinoshita@pu-toyama.ac.jp
Adv. Sci. Technol. Eng. Syst. J. 5(2), 757-761 (2020); ![]() DOI: 10.25046/aj050294
DOI: 10.25046/aj050294
Keywords: Dementia, circadian rhythm, Actigraph, translation error, Hurst exponent.

Export Citations
Dementia is one of the three primary diseases that increases the level of nursing care required for the elderly. Dementia can lead to an increased burden not only on those who have contracted it, but also their families and the surrounding environment; initiatives for preventing dementia and slowing the decline of cognitive function are expected to reduce these burdens. This study focuses on phototherapy as an alternative non-pharmaceutical treatment for dementia. This study examined the activity of elderly dementia patients to determine the effect of phototherapy on their circadian rhythms. A total of 15 dementia patients within the age range of 86.3 ± 6.2, were selected as subjects, and the data were collected using a wristwatch data logger (Actiwatch2). The phototherapy consisted of 5,500 lux intensity light exposure from 7 a.m. to 9 a.m., and data measurements were taken for three 14-day periods, i.e., before, during, and after phototherapy. Frequency analysis using discrete Fourier transform and nonlinear analysis called Hurst exponential and translation error were used to analyze the activity data. Compared to before phototherapy, the Hurst exponent values during phototherapy showed a significant increase in value (p<0.05) and the translation error values showed a trend of decreasing. The increase in the Hurst exponent values seen in the present experiment suggests that phototherapy may have improved the cyclicality of the circadian rhythm. However, when the phototherapy ended, the subjects’ Hurst exponent values returned to the previous levels observed prior to phototherapy, and no significant differences in data were found before or after phototherapy. Thus, phototherapy, a possible treatment of sleep disorders, is also effective in promoting regularity in circadian rhythms in elderly dementia patients to a certain extent.
Received: 25 March 2020, Accepted: 16 April 2020, Published Online: 20 April 2020
1. Introduction
In recent years, advances in medical technology and an improved nutritional standing of individuals has increased life expectancies globally. As the population is aging, the number of elderly people who require nursing care is increasing. Additionally, the cost of care, including insurance premiums, is also increasing, which is problematic. Dementia is one of the three main diseases that leads to nursing care requirements for the elderly. Dementia is defined as “a condition in which cognitive functions that had previously reached normal levels continually decline as a result of an acquired brain disorder, inhibiting the sufferer’s day-to-day activities and social life.” However, the method for diagnosing dementia is not defined, and current medical science does not consider complete recovery from dementia as a possibility [1]. Because dementia results in an increased physical, mental, and emotional burden not only on the patient who contracts it, but also on their families and surrounding communities, there are increasing expectations for initiatives to prevent the onset of dementia and delay the decline of cognitive function.
The symptoms of dementia can be broadly categorized into two groups: core symptoms and peripheral symptoms. Core symptoms are the main symptoms of dementia, and they include disorders of thinking, decision-making, and executive functions. Peripheral symptoms related to these include behavioral and psychological symptoms, such as hallucinations, delusions, wandering, aggressive language, and violence. These symptoms are also called behavioral and psychological symptoms of dementia (BPSD). While visual hallucinations are associated with Lewy body dementia, and roaming behavior is associated with frontotemporal dementia, BPSD and core symptoms of dementia are not clearly separated by disease type [2-4]. Currently, a complete recovery from dementia is considered impossible; the core symptoms of dementia cannot be completely cured. Depending on whether appropriate pharmaceutical therapy and care methods are implemented, BPSD can be reduced in some cases and exacerbated in others [5]. Accordingly, the goals of rehabilitation implemented for dementia patients include psychological stability and improvement of BPSD.
A variety of non-pharmaceutical treatments for dementia have been proposed. Some examples include therapeutic exercise, reminiscence therapy, phototherapy, and music therapy. However, therapeutic exercise is the only effective treatment with established evidence. This is not because there is a lack of evidence for other treatments, but because not enough qualitative research has been conducted to derive evidence; as a result, they cannot be properly evaluated [6]. This study focuses on accumulating evidence for phototherapy as an alternative non-pharmaceutical treatment.
Phototherapy is a treatment method used for sleep disorders. Having 1-2 hours of exposure to a bright light over 2,500 lux in intensity, the central nervous system’s production of the sleep hormone melatonin is suppressed, which has the effect of restoring a biological circadian rhythm. Because the human biological clock consists of approximately a 25-hour cycle, if individuals live in an environment without a sense of time, the phases of the circadian rhythm of body temperature controlled by melatonin and other hormones fall behind as the days progress [7, 8]. When light is transmitted from the retina to the supraoptic nucleus via the optic nerve, this information is used to adjust the phases of the biological clock. High-intensity light is the most powerful factor contributing to the adjustment of the human biological clock to a 24-hour circadian rhythm [9,10]. Because elderly dementia patients have trouble maintaining their sleep patterns due to factors such as frequently waking from sleep, they are at a high risk for disrupted sleep-wake patterns [11]. This is due to age-related changes in the supraoptic nucleus and decreased secretion of melatonin. Prior research suggests that exposure to high-intensity light in the early morning hours, when the circadian fluctuation of the body temperature shifts from falling to rising, can sync the sleep-wake patterns of dementia patients to an afternoon-night rhythm [12, 13]. However, the majority of these existing studies used questionnaires and sleep journals for the evaluation of sleep patterns after phototherapy, and there are few examples of quantitative data analyzed using numerical methods.
This study evaluates the effects of phototherapy on the circadian rhythms of elderly dementia patients using a portable activity measurement device system called Actigraph. The Actigraph system is being used in many sleep studies in recent years [16, 17]. Determining whether subjects are awake or asleep based on the body movement measurement results of the Actigraph system has a high rate of correlation to a polysomnogram [14, 15]; the device is also easy to wear, reducing the burden on both, subjects and researchers, making it easier to take measurements for a prolonged time period. In this study, activity volume measurements were taken for 14 days prior to, during, and after phototherapy, for a total of 42 days. This was then evaluated using frequency and non-linear analysis.
2. Materials and Methods
Study participants included a total of 15 elderly dementia patient residents at geriatric health service facilities within Toyama Prefecture, ages (mean ± SD) 86.3 ± 6.2. The study was thoroughly explained to the subjects in advance, and they gave their written consent to participate. In addition, in cases where it was uncertain whether this consent was truly based on the will of the subject, consent was received by proxy. This study was implemented after obtaining approval from the Toyama Prefectural University Research Ethics Committee (R1-2).
Actigraph measurements were taken using a wristwatch type data logger, an Actiwatch2 by Philips Respironics. The Actiwatch2 uses an accelerometer signal for the level and frequency of body movements, and can record body movement activity counts in intervals of 60 s. For each subject, the study protocol consisted of activity count measurements for a 42-day period. This was broken up into three 14-day blocks before, during, and after phototherapy. Measurements started at 3:00 p.m. for all subjects, and during the phototherapy block, they were exposed to a 5,500 lux intensity light from 7:00 a.m. to 9:00 a.m.
3. Data Analysis
The chronological data for activity counts (below: AC chronological data) was analyzed using discrete Fourier transform (DFT) for frequency analysis, and both Hurst exponent and translation error methods were used for nonlinear analysis.
The translation error values estimated using the Wayland algorithm were used as quantitative evaluation indicators for the smoothness of the embedded attractor trajectory in the phase space [18, 19]. Although there exists an alternative method for focusing on the smoothness of the embedded attractor trajectory in the phase space called the Grassberger-Procaccia algorithm, it has drawbacks including the requirement of a large volume of data, as well as being sensitive to noise and interference in stacked chronological data.
An outline of the Wayland algorithm is shown below. For a vector at time , the closest vector may be determined, Followed by measuring the Euclidean distance between the two vectors. These vectors are written as: . When time step has elapsed, moves to . At this time, the change in trajectory over time is approximated as . If the direction dispersion of is calculated, the degree to which the directions are in line and the time development appears deterministic, can be quantitatively evaluated. Equation (1) provides directional variance:
where is the translation error. In order to determine the error arising from the selection of , randomly selected values of must be used to calculate the median value of a total of times, and the mean of these median values expresses the translation error. For this study, the coefficient conditions selected were ( , , ) = (51, 4, 10). If the trajectory of the attractor reconstructed in the embedded space is smooth, this shows that the chronological data is deterministic. Translation error takes a positive value, and a value close to 0 indicates that the mathematical model for generation of the chronological data is deterministic, while a large value indicates a probabilistic model. Specifically when the target is the Brownian motion, the translation error value is expected to equal 1.
Next, the Hurst exponents are a scale for bias in non-linear Brownian motion; they indicate the extent to which data deviates from the Brownian motion, expressing the degree of bias in changing trends [20]-[21]. If the Hurst exponent value is 0.5, this indicates Brownian motion in chronological data. This is the base value, and values closer to 0 indicate a discontinuity while values closer to 1 indicate a continuity. R/S analysis is one of the analysis methods Hurst devised for calculating the Hurst exponent. Eq. (3) is provided as a rudimentary model for explaining the random walk process in Brownian motion:

where is an arbitrary time period and represents the fluctuation range during that time period. With respect to Eq. (3), Hurst divided the range of observed values by standard deviation intervals in order to standardize the applicable time scale. This allows for the creation of a dimensionless scale that can be used for comparisons. Hurst provided Eq. (4) as a generalized version:
Here, is the range of deviation within an arbitrary time period, is the standard deviation, expresses the Hurst exponent, and is a constant. In this study, values corresponding to for both logarithmic graphs were plotted, and a straight line was applied to the scatter plots drawn using the least-squares method. The slope of this line was taken as an estimated value for . In addition, intervals ranging from 400 to 600 units of 60 were used as the time period T values for R/S analysis.
Because the AC chronological data acquired in this study was sampled in 60-s increments, there were a total of 20,160 chronological data points for each 14-day block. For each of the 14-day blocks, before, during, and after phototherapy, a 720-point width moving average was calculated after the high frequency components were removed from the data.
4. Results
Figure 1 depicts an example of a typical AC chronological data series recorded by the Actigram system for the 14-day block before phototherapy. Among the elderly dementia patients, although there were some subjects whose activity counts showed regular activity (Figure 1a, Figure 1c), data for others confirmed irregular activity (Figure 1b, Figure 1d). Next, DFT was used to analyze the frequency of the waveforms for AC chronological data recorded by the Actigram system before, during, and after phototherapy time blocks. In addition, the power spectrum shown in Figure 2 is normalized so that the total equals 1. Among the elderly subjects with regular circadian rhythms, the peak frequency of the power spectrum was close to 1 cycle per day (cpd). For those with irregular circadian rhythms, however, no power spectrum peak frequency near 1 cpd could be confirmed by visual examination. Using this data, the power spectral density (PSD) range before, during, and after phototherapy was calculated as 0.8-1.2 cpd. The mean value of results for the 15 subjects are depicted in Figure 3 below. The mean values for PSD fluctuated by around 0.17, decreasing during the phototherapy time block. Next, a one-way analysis of variance was conducted for each of the three time blocks, and when a main effect was observed, multiple comparisons were performed using the Bonferroni method. Results showed significant lower mean values for PSD during phototherapy than those before the phototherapy time blocks (p < 0.05).
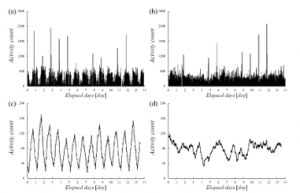
Figure 1: Typical example of AC chronological data recorded by the Actigram (during the 14-day period prior to phototherapy). Example of an elderly person with a regular (a) and irregular (b) circadian rhythm. After moving average for a regular (c) and irregular (d) circadian rhythm.
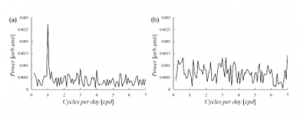
Figure 2: AC time series frequency analysis (14-day period prior to phototherapy). Example of an elderly person with a regular (a), and irregular (b) circadian rhythm.
Next, the translation error and Hurst exponent values for the AC chronological data for the three 14-day periods before, during, and after phototherapy were used for analysis. The mean results for the 15 subjects are depicted in Figure 4 and Figure 5. The translation error before the phototherapy block was around 0.32, with fluctuating values. However, the translation error decreased to around 0.28 during the phototherapy block, then increased again to approximately 0.32 following the phototherapy block. This was followed by a one-way analysis of variance for the values before, during, and after phototherapy. The results indicated insignificant effects for translation error. The Hurst exponent value for the block before phototherapy was approximately 0.8, with fluctuating values. However, the exponent increased to approximately 0.89 during the phototherapy block, then finally decreased to approximately 0.82 in the after phototherapy block. Next, a one-way analysis of variance was conducted for each of the three time blocks, and when a significant effect was observed, multiple comparisons were performed using the Bonferroni method. The results indicated a significant increase in the Hurst exponent values during the phototherapy block compared to the before phototherapy block (p < 0.05).
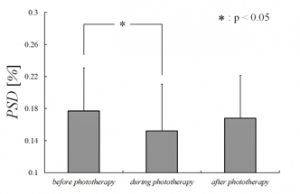
Figure 3: PSD mean values (mean ± SD)
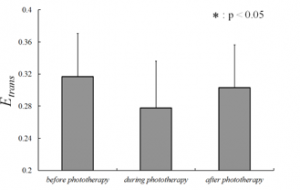
Figure 4: Translation error mean values (mean ± SD)
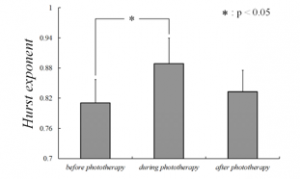
Figure 5: Hurst exponent mean values (mean ± SD)
5. Discussion
The effectiveness of high-intensity phototherapy for the treatment of seasonal affective disorder (SAD) was first reported in 1982 by Rosenthal et al. Since then, it has become the most popular treatment for SAD. High-intensity phototherapy modifies the phases of circadian rhythm, and it has been reported effective for sleep disorders related to old age, as well as dementia [22]. On the other hand, according to the “2017 Dementia Patient Treatment Guidelines” (Japan Society of Neurology), the only non-pharmaceutical therapy for dementia with established evidence for its effectiveness is therapeutic exercise. Although a variety of non-pharmaceutical treatment methods are being conducted at many facilities and day services, evidence for their effectiveness is currently weak across the board. However, this is not because the effectiveness of other non-pharmaceutical treatments is poor, but because there has been limited scientific evaluation of these treatments until now. Additionally, the majority of prior studies relative to phototherapy used questionnaires and sleep journals for the evaluation of sleep patterns after treatment, and there are few examples of quantitative data analyzed using numerical methods.
This study conducted an experiment focused on quantitative chronological activity data for before and after phototherapy as an initiative for accumulating evidence on these non-pharmaceutical treatments. Quantitative chronological activity data measurements were taken using a wristwatch type data logger, Actiwatch2made by Philips Respironics, for a total of 15 subjects, all elderly dementia patient residents at geriatric health service facilities at Toyama Prefecture. Frequency analysis using discrete Fourier transform and nonlinear analysis called Hurst exponential and translation error were used to analyze the activity data. The periodicity and regularity of the time series can be quantitatively confirmed by using these analytical indicators. Data measurements were carried out for 14 days each before, during, and after phototherapy. The results indicated that both, PSD and Hurst exponent values for 0.8-1.2 cpd data either decreased or increased during phototherapy compared to before phototherapy (p < 0.05). Hurst exponents express deviation from Brownian motion, and can be used to evaluate the continuity of chronological data. Continuity refers to the characteristic of rising trends continuing to rise, and falling trends continuing to fall in chronological data values. In the case of dementia, stronger symptoms are expected to cause more of an extreme failure of the circadian rhythm cycle, and the increased Hurst exponent values seen in this experiment suggest that phototherapy could have improved the circadian rhythm cycle in the subjects. However, when phototherapy ended, subjects’ Hurst exponent values returned to the previous levels observed prior to phototherapy, and no significant differences were found when comparing data before and after phototherapy. This trend was also confirmed by the PSD values for 0.8-1.2 cpd data. The translation error values were approximately 0.3 with some fluctuation, and determinism in the patients’ activity was confirmed. Although no significant differences were found in the measurement data from before and after phototherapy, translation error values tended to decrease during phototherapy. This indicates that the determinism of the chronological data increased, suggesting that the circadian rhythms of the elderly dementia patients became smoother. Although the peak frequency of the power spectrum for elderly subjects with regular circadian rhythms was around 1 cpd, as in the healthy subjects, no power spectrum peak could be confirmed for the irregular rhythm subjects. Because the effects of phototherapy may differ between the regular and irregular circadian rhythm subjects, there should be an increased number of subjects for future studies to evaluate methods, such as circadian rhythm periodicity and MMSE scores, and further divide elderly dementia patients into groups for analysis.
6. Conclusions
This study collected quantitative chronological activity data for three 14-day periods before, during, and after phototherapy, for a total of 42 days of measurements. Frequency analysis and nonlinear analysis were then used for evaluation. The results confirmed that phototherapy, a treatment method used for sleep disorders, is also effective to a certain extent for promoting a regular circadian rhythm in elderly dementia patients. Additionally, the study confirmed that this effect was lost when phototherapy ended. Furthermore, the power spectrum data acquired from the frequency analysis confirmed that elderly dementia patients can be grouped with both, regular and irregular circadian rhythms. Further consideration is necessary to determine whether phototherapy is effective for both groups in light of control experiments. Future studies may use methods, such as circadian rhythm periodicity and Mini-Mental State Examination (MMSE) scores, to further divide the elderly dementia patients into groups. Moreover, the trends confirmed in this study must also be evaluated to determine whether they have the potential for preventing dementia and delaying cognitive decline.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgment
This work was supported by JSPS KAKENHI Grant Number 19K11232.
- Dementia Diagnosis and Treatment Guideline Planning Committee (supervised by the Japanese Society of Neurology): 2017 Dementia Diagnosis and Treatment Guidelines, Igaku Shoin, Tokyo, 2017.
- International Psychogeriatric Association (translation supervised by the Japanese Psychogeriatric Society): Dementia behavioral and psychological BPSD (2nd Edition), ALTA Publishing, 2013.
- Finkel, Costa E Silva JA, G. Cohen, S. Miller, N. Sartorius, “Behavioral and Psychological Symptoms of Dementia: A Consensus Statement on Current Knowledge and Implications for Research and Treatment”, International Psychogeriatric Association, 1998.
- Matsushita, “Focusing on occupational therapy for improving daily activities and QOL as an approach for revalidation”, Bulletin of Morinomiya University of Medical Sciences, 11, 25-32, 2017.
- Yamaguchi, “Definition, clinical issues and etiology of BPSD”, Tokyo Journal of Dementia Care Research, 2, 1-16, 2018.
- Sato, “The present and future of non-pharmaceutical treatments for dementia”, Cognitive Neuroscience, 15(3), 207-213, 2014.
- J. Kennaway, C.F. Van Dorp, “Free-running rhythms of melatonin, cortisol, electrolytes, and sleep in humans in Antarctica.”, Am. J. Physiol., 260(6), R1137-1144, 1991.
- A. Wever: The Circadian System of Man -Results of Experiments Under Temporal Isolation-, Springer-Verlag, New-York, 1979.
- S. Campbell, P.J. Murphy, C. J. van den Heuvel, et al., “Etiology and treatment of intrinsic circadian rhythm sleep disorders.”, Sleep Med Rev., 3(3), 179-200. 1999.
- S. Campbell, M. Terman, A.J. Lewy, et al. “Light treatment for sleep disorders: consensus report. V. Age-related disturbances.”, J Biol Rhythms., 10(2), 151-154, 1995.
- The Japan Foundation for Aging and Health: Sleep and its disorders in the elderly, 2016 essay collection, Aichi, 2017.
- A. Dowling, E.M. Hubbard, J. Mastick, et al. “Effect of morning bright light treatment for rest-activity disruption in institutionalized patients with severe Alzheimer’s disease.”, International Psychogeriatric Association, 17(2), 221-236, 2005.
- Ito, H. Yamadera, R. Ito, et al., “Effects of high intensity phototherapy on the cognitive impairment of patients with Alzheimer’s type dementia”, Journal of Nihon University Medical Association, 66(4), 229-238, 1999.
- J. Cole, D.F. Kripke, W. Gruen, et al., “Automatic sleep/wake identification from wrist activity.”, Sleep, 15(5), 461-469, 1992.
- Sadeh, “The role and validity of actigraphy in sleep medicine: an update.”, Sleep Med. Rev., 15(4), 259-267, 2011.
- The Japanese Society of Sleep Research: Japanese Sleep Research Handbook, Asakura Shoten, Tokyo, 1994.
- Yamanaka, A. Nakada, “Case study analysis of the effects of the implementation of day activities by student volunteers on the activity and sleep of elderly dementia patients using Actigram”, Journal of Japanese Society for Dementia Care, 7(3), 535-545, 2008.
- Wayland, D. Bromley, D. Pickett, “Recognizing determinism in a time series”, Phys. Rev. Lett, 70, 580-582, 1993.
- Takada, Y. Simizu, H. Hoshita, et al., “Wayland tests for differenced time series could evaluate degrees of visible determinism”, Bulletin of Society for Science on Form, 17(3), 301-310, 2005.
- E. Hurs, R.P. Black. Y.M. Simaika: Long-term storage: an experimental study Constable Press, London, 1965.
- Oishi, M. Takubo, “Chronological data identification and R/S analysis, new perspectives on data analysis”, Management Research, 10(3), 449-482, 1997.
- Rosenthal NE, Sack DA, Gillin JC, Lewy FK, Goodwin FK, Davenport Y, Mueller PS, New-some DA, Wehr TA: Seasonal affective dis-orders: A description of the syndrome and preliminary findings with light therapy. Arch Gen Psychiat 41: 72-80, 1984.