An Exploratory Qualitative Study of the Influence of Hospital Logistics Factors on Quality of Care and Patient Satisfaction at Public Hospitals in Morocco
Volume 4, Issue 6, Page No 414-422, 2019
Author’s Name: Youness Frichia), Fouad Jawab, Said Boutahari
View Affiliations
Industrial Technologies and Services, High School of Technology, Sidi Mohamed Ben Abdellah University, Fez 30 000, Morocco
a)Author to whom correspondence should be addressed. E-mail: youness.frichi@usmba.ac.ma
Adv. Sci. Technol. Eng. Syst. J. 4(6), 414-422 (2019); ![]() DOI: 10.25046/aj040652
DOI: 10.25046/aj040652
Keywords: Hospital logistics, Quality of care, Patient satisfaction

Export Citations
The purpose of this qualitative research was to explore the influence of hospital logistics on quality of care and patient satisfaction. Hospital logistics was assessed by considering five factors in the patient pathway, namely: physical accessibility of care, waiting time, consultation time, administrative procedures and hospital hotel services. Semi-structured interviews were conducted, following an interview guide, with two categories of participants: patients and healthcare professionals. The interviews were transcribed and then a thematic analysis method was conducted using QSR NVivo 10 software. Results showed that hospital logistics has a direct impact on quality of care and patient satisfaction. All the participants’ testimonies highlighted the critical and crucial role that hospital logistics plays in the perception of quality of care and patient satisfaction. It is recommended to pay great attention to hospital logistics activities in order to improve quality and satisfaction.
Received: 11 November 2019, Accepted: 09 December 2019, Published Online: 25 December 2019
1. Introduction
This study is the extension of a previous study entitled “Elaboration of an association matrix of satisfaction factors in healthcare facilities and hospital logistics activities” in 2018 International Colloquium on Logistics and Supply Chain Management (LOGISTIQUA). The previous study examined the effect of hospital logistics factors on healthcare quality and patient satisfaction [1]. It was found, through a literature review, that patient satisfaction is influenced by several factors including hospital logistics factors [1]. The objective of this study is to support empirically these findings in order to better understand the effect of hospital logistics on quality of care and patient satisfaction. Given that the Moroccan Ministry of Health’s new strategy (Ministry of Health (2018) “Plan Santé 2025“, https://www.sante.gov.ma/Pages/actualites.aspx?IDActu=276) aims to ensure that healthcare services are of high quality and meet patients’ needs, it was decided to conduct this empirical study in the Moroccan context. So, the contribution of this article is fully in line with this perspective by exploring the role of hospital logistics as a lever for quality and satisfaction. The health system in Morocco is structured in two sectors [2]:
- The public health sector: comprises healthcare services of the Ministry of Health, Defense department, and local authorities. Healthcare facilities under the Ministry of Health are Basic Healthcare Centers (BHC), Provincial Hospital Centers (PHC), Regional Hospital Centers (RHC), and University Hospital Centers (UHC).
- The private health sector: incorporates the private for-profit sub-sector that includes hospital clinics, dental surgery, pharmacies, etc., and the private not-for-profit sub-sector that includes healthcare services of the National Fund for Social Security, the National Fund of Social Welfare Bodies, the Moroccan Red Crescent, and non-governmental organizations.
The focus of this paper is on the public sector, particularly the healthcare services of the Ministry of Health provided at hospitals. The remainder of this article is organized as follows. Section 2 highlights the background of this research. Section 3 describes the methodology for data collection and analysis. Section 4 presents the results of the study. Section 5 provides a discussion of the main findings. Finally, the paper’s limitation and future research, as well as conclusions are presented in sections 6 and 7 respectively.
2. Background
2.1. Quality of care
Quality of care is defined in different ways in the literature. According to Donabedian [3], high-quality care is the kind of care that is expected to maximize an inclusive measure of patient welfare after one has taken into account the balance of expected gains and losses that attend the process of care in all its parts. From this definition, two aspects of quality of care might be distinguished: (1) technical quality that refers to medical practices and clinical outcomes; (2) quality of the care delivery processes and how the patient receives the service [4]. This second aspect can be assessed by measuring patient satisfaction [5]. However, some authors argued that patient satisfaction is not sufficient and must include other stakeholders’ points of view [6]. In this paper, quality of care is considered only in terms of patient satisfaction.
2.2. Patient satisfaction
Patient satisfaction is defined as an assessment that reflects the perceived differences between the patient’s expectations and what is actually received during the process of care [7]. It is considered to be the main indicator of quality of care. The objective of patient satisfaction studies is to understand the factors associated with satisfaction and whose improvement could enhance the quality of care [8]. Factors thought to be related to patient satisfaction include patient sociodemographic and health status characteristics [9], expectations concerning medical care [10], caregivers’ attitudes and behaviors [11], waiting time [12], consultation time [13], healthcare accessibility [14], administrative procedures [15], and hospital hotel services [16]. It was concluded from previous studies that some of these factors fall within the scope of hospital logistics [17].
2.3. Hospital logistics
Hospital logistics is a set of processes that exchange physical, information and financial flows in order to ensure all the necessary conditions to provide patients with a better quality service [18]. This definition reflects the scope of hospital logistics, which includes all the support activities that are necessary for providing care: scheduling, forecasting, transportation, procurement, distribution, replenishment, information system, patient flow, catering, laundry, waste management, maintenance, etc. [19]. Over the last few decades, hospital logistics has received a great deal of interest from researchers. It is recognized to play an important role in improving the quality of care and patient satisfaction [20]. Indeed, many factors of patient satisfaction such as waiting time, consultation time, physical accessibility of care, hospital hotel services, and administrative procedures depend on the effectiveness of hospital logistics activities.
2.4. Interactions between hospital logistics and patient satisfaction
As mentioned above, several patient satisfaction factors fall within the scope of hospital logistics, including:
- Waiting time: is identified by most studies as a factor that has a strong impact on satisfaction. A long waiting time may result from several causes, in particular, the inadequacy between the available resources (staff, operating rooms, hospital beds, drugs, equipment, etc.) and the patient flow [21,22]. This inadequacy is mainly due to a lack of planning and coordination in service delivery or because hospital resources are allocated in a way that is not dynamic and does not take into account the growing need for care [23,24].
- Consultation time: is the time spent with the caregiver. The longer the consultation time, the more satisfied patients are [13]. Consultation time is sometimes reduced because caregivers spend a huge amount of their time managing administrative and logistical matters, which reduces the time available for patients. Estimates indicate that a nurse spends between 30% and 34% of her time on logistical and administrative activities [25,26]. The availability of caregivers could be increased by freeing them from logistical and administrative tasks that consume a lot of their time [27].
- Physical accessibility: the physical accessibility of healthcare services depends on several logistics factors both outside and inside healthcare facilities. The patient’s arrival is first ensured by adapted means of transportation such as ambulances. The availability of ambulances requires good management (maintenance, fuel allocation, human resources, equipment, etc.). Second, at the healthcare facility, access to care requires the availability of the right human resources with the right skills in the right place, which is conditioned by optimal time management, medical intervention planning, staff assignment, etc. [28]. Third, the availability of material resources such as operating rooms, medical analysis and radiology laboratories, technical equipment, etc., depends on the effectiveness of planning and scheduling operations, coordination between healthcare teams and maintenance activities. Also, the availability of medical supplies such as drugs and sterile medical devices (needles, syringes, gloves, etc.) is dependent on the effectiveness of procurement and inventory management systems [26].
- Hospital hotel services: such as catering, cleanliness, laundry, and accommodation conditions of patients stay at the hospital. Satisfaction surveys showed that the highest patient dissatisfaction was reported regarding hoteling services [7,29]. Adequate hospital hotel services require better planning and coordination between the different teams. For instance, the catering activity requires an efficient supply system to ensure fresh meals at the right time, as well as better coordination between the catering service and the care teams to consider the nutritional specificities of each patient. The cleaning activity is responsible for the cleanliness of the healthcare environment (e.g. wards, toilets, waiting areas, etc.). It assumes cleaning the hospital areas at regular intervals and whenever necessary, making cleaning supplies available in sufficient quantities in the right places, as well as adequate management of hospital wastes. The laundry activity provides care units with clean linens, towels, and staff uniforms, which ensures comfort, hygiene, and safety for hospitalized patients. In this respect, well-adapted logistics circuits are essential: definition of storage areas for clean and soiled linen, towels and linen transportation, operations’ planning and sequencing (disinfection, washing, rinsing, and drying) [30]. It is worth mentioning that hospital hotel activities are often outsourced, therefore their effectiveness depends on outsourcers’ performance.
- Administrative procedures: administrative formalities related to patient admission, treatment, and discharge are associated with patient satisfaction [31]. These procedures can be optimized and simplified through better information flow management. The use of hospital information systems (HIS), including the implementation of electronic medical records is of great help [32].
Table 1: Semi-structured interview guide
| Themes | Questions asked during the interviews | |
| Quality of care | Can you describe what quality of care is all about? | |
| Patient satisfaction | What makes a patient satisfied with hospital services?
What are the determinants/factors of patient satisfaction? |
|
| Hospital logistics factors | Waiting time | Can you describe the importance of delay in medical care and its influence on patient satisfaction and quality of care? |
| Consultation time | To what extent is consultation time important for quality of care and patient satisfaction?
Why is the consultation time sometimes reduced? |
|
| Physical accessibility | How important is the ease of physical access to care?
What are the factors that influence the physical accessibility of care? |
|
| Hospital hotel services | To what extent are hospital hotel services essential (cleanliness, laundry, comfort, catering, etc.)? | |
| Administrative procedures | Can you describe the importance of organization, clarity, and ease of administrative procedures? | |
3. Methods
Given the exploratory nature of this study, a qualitative approach was employed. Qualitative approaches are appropriate for a comprehensive exploration of participants’ perceptions and experiences. Some of the main techniques for collecting qualitative data in healthcare researches include individual interviews, focus groups, and observation [33]. In this study, semi-structured individual interviews are used. This choice is explained by the study’s objective that consists of identifying and exploring the different perceptions of healthcare professionals and patients regarding the importance of the above-mentioned hospital logistics factors in ensuring quality of care and patient satisfaction. Data collection and analysis were based on steps described by Imbert [34]: development of the interview guide, participant selection, interviewing participants, and data analysis.
3.1. Interview guide
Semi-structured interviews collect data by interviewing participants face-to-face using an interview guide which contains the list of questions or topics to be covered. The interview guide developed here contained open-ended questions, that are structured in seven themes as shown in Table 1. Conversations were initiated by asking general questions about the quality of care and patient satisfaction and then questions become specific about hospital logistics factors.
3.2. Participant selection
Two categories of participants were included in the study: the healthcare professional category and the patient category. The first includes physicians and healthcare managers, while the second is composed of former patients who have been hospitalized in public hospitals at least once in the last three months. In total, 5 participants from each category were included, they were from three types of public hospitals: University Hospital Center (UHC), Regional Hospital Center (RHC), and Provincial Hospital Center (PHC) (Table 2).
Table 2: Participants in semi-directive interviews
| Participant | Experience | Hospital | City | |
| Healthcare professional category | ID1: Quality manager | 13 years | RHC | Fez |
| ID2: Head of Medical Affairs
Department |
17 years | RHC | Fez | |
| ID3: Logistics manager | 16 years | RHC | Fez | |
| ID4: Head of Performance
Evaluation Department |
24 years | UHC | Rabat | |
| ID5: Emergency physician | 6 years | PHC | Casablanca | |
| Patient category | ID6: Patient 1 | 3-day inpatient | UHC | Fez |
| ID7: Patient 2 | 2-day inpatient | UHC | Fez | |
| ID8: Patient 3 | 3-day inpatient | RHC | Fez | |
| ID9: Patient 4 | 2-day inpatient | RHC | Fez | |
| ID10: Patient 5 | 3-day inpatient | PHC | Fez | |
3.3. Interviewing participants
The richness of semi-structured interview data depends on the trust relationship between the interviewer and the interviewees [34]. With this in mind, the interviews were started by an introduction to explain the objective of the study and to assure participants of the anonymity and confidentiality of their data, as well as to ask for permission to record the interviews. Healthcare professionals working in Fez city were met individually at their place of work. For those outside of Fez, the interviews were conducted by phone. Concerning the participants from the patient category, the exchanges were face-to-face.
All interviews were started by asking questions about the quality of care and patient satisfaction regarding hospital services. Subsequently, participants were asked for their opinions on hospital logistics factors as illustrated in the interview guide. Conversations were sometimes deepened for clarification purposes by asking why or how questions [35]. At the end of each interview, the interviewee was given the opportunity to add and discuss anything he or she thought was relevant or important and had not been discussed during the interview. Interviews took place during September and October 2019 and lasted between 30 to 60 minutes.
3.4. Data analysis
A thematic analysis was carried out for data analysis. It is the most common method for qualitative data analysis. It consists of identifying, analyzing, reporting patterns within data, and organizing them into themes, whether predefined or emerging themes [36]. In this study, themes are already defined and correspond to quality of care, patient satisfaction, and hospital logistics factors.
Recordings transcription is the first step in data analysis [36]. For that purpose, all interviews were transcribed using Google Docs’ voice typing tool. The second step is coding interesting features of the textual data. It consists of assigning codes or labels, which are summative and essence-capturing attributes, for a portion of data [37]. Since the themes in this study are already defined, the coding method is a combination of descriptive coding, to describe and summarize the content of a sentence or a portion of the data, sub-coding to classify and categorize the codes into families, themeing the data to assign codes to predefined themes, and attribute coding to distinguish between healthcare professional participants and patient participants [37]. The coding process was performed using QSR NVivo 10 qualitative data analysis software.
4. Results
4.1. Quality of care
Participants from the healthcare professional category have defined the quality of care using criteria such as effectiveness, efficiency, and compliance with standards “quality of care consists of providing healthcare according to standards and effective cost control” (participant ID1). Other criteria were also mentioned including resource availability, accessibility, and responsiveness. For participants from the patient category, quality of care is attributed to good staff attitude and appropriate pain management within a short time frame “quality of care requires a rapid healthcare delivery; the patient should not wait for a long time to be examined and treated” (participant ID10). Participants have also insisted on the availability of skilled human resources, sufficient and functional material resources “quality of care is conditioned by the availability of skilled doctors as well as technical equipment in sufficient quantity and quality” (participant ID5).
4.2. Patient satisfaction
Interviewees from the healthcare professional category indicated that patients are satisfied when their expressed needs are met, which is not accurate. According to participants, caregivers should satisfy the real need resulting from the medical diagnosis “to satisfy the patient, it is necessary to meet his or her expressed needs, which do not necessarily coincide with the real needs. The patient is unable to define the real needs” (participant ID2). They claimed that patient satisfaction does not depend on the technical quality of care but tends to focus on the tangible aspects of the service “from our experience in satisfaction surveys, we observe that patient satisfaction is not related to the technical aspects of care, but rather to support functions such as catering, cleaning, etc. This is mainly due to the fact that patients are unable to judge the technical care” (participant ID3). Interviewees from the patient category insisted on the staff attitude as a determinant of satisfaction “patients are satisfied if they are physically and psychologically relieved, this depends on the behavior and attitude of the staff” (participant ID6); “patients are satisfied when they find a welcoming staff that soothe patients’ anxiety and reduce the stress level” (participant ID9). They also insisted on the importance of the availability of care providers, equipment and supplies, and the reduction of waiting times “For the patient to be satisfied, healthcare must be available, staff behave well and treatment times are rapid” (participant ID8).
4.3. Hospital logistics factors
To meet the objective of this exploratory study, we have reported in Table 3, the hospital logistics factors/themes and their corresponding codes.
Table 3: code categories of hospital logistics factors
| Themes/ Factors | Code categories |
| Physical accessibility | Location of the healthcare facility |
| Medical transportation | |
| Hospital reception | |
| Signs and architecture | |
| Availability of human resources | |
| Availability of material resources | |
| Waiting time | Appointment scheduling |
| Waiting time | |
| capacity-demand gap | |
| Patient flow | |
| Non-compliance with the gatekeeping system | |
| Consultation time | Workload |
| Performing non-professional tasks | |
| Hospital hotel services | Cleanliness/ hygiene/ laundry |
| Comfort | |
| Catering | |
| Outsourcing | |
| Administrative procedures | Rules and regulations |
| Clarity of procedures |
These themes were raised by participants to different degrees. The frequency of codes under each theme according to their appearance in the corpus was generated by QSR NVivo and reported in the matrix in Figure 1. This matrix allows the content of qualitative data to be visualized and quantified.
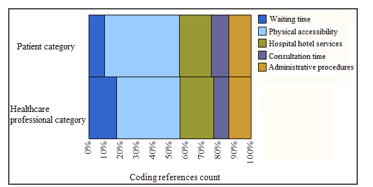 Figure 1: Matrix coding query – results preview
Figure 1: Matrix coding query – results preview
4.3.1. Physical accessibility
Figure 1 shows that the physical accessibility theme is the most discussed by both patient and healthcare professional participants. This theme includes a set of physical elements that are necessary to receive healthcare services. Participants agreed on the critical aspect of physical accessibility in relation to quality of care and patient satisfaction “any accessibility problem prevents the patient from seeking care, which can worsen and harm his or her health status” (participant ID1). Their perceptions are structured into six elements of the care pathway: location of the healthcare facility, medical transportation, hospital reception, signs and architecture, availability of human and material resources. Figure 2 shows the number of coded references for each of these elements. It can be seen that the availability of human and material resources are the most frequently mentioned elements.
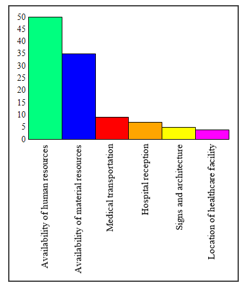 Figure 2: Physical accessibility – number of coding references per element
Figure 2: Physical accessibility – number of coding references per element
- Location of the healthcare facility
The first step towards receiving healthcare services is to access the healthcare facility, which depends on its geographical location. Participants believe that healthcare access is easier when the healthcare facility is accessible by public transportation “obviously the geographical location of the healthcare facility can facilitate or hinder access to healthcare” (participant ID5); “If the hospital is located in the city center and accessible by public transportation such as buses and taxis, healthcare becomes easily accessible” (participant ID 7).
- Medical transportation
Medical transportation ensures patient access to healthcare facilities. Despite its importance, medical transportation is considered to be the weakest link in the healthcare supply chain. Indeed, most participants made a negative assessment of medical transportation. It is criticized for its inefficiency, poor management as well as the multiplicity of the involved actors without a real coordination “when I had my leg broken during a football match, my family did not call an ambulance because it is rare when ambulance services respond, and if they do, they are often late” (participant ID7); “the medical transportation system is ill at ease because it is poorly managed. Sometimes ambulances are available but inaccessible. There are several problems, including lack of coordination between actors, maintenance problems, insufficient fuel supply, regulations, etc.” (participant ID4).
- Hospital reception
Patients’ initial impression of healthcare services depends on the quality of the hospital reception. It is the first contact with the healthcare facility. At this stage, the patient or his/her family seeks information about the admission and treatment process. Therefore, a good hospital reception fosters patients’ adherence to treatment and ensures continuity of care “the quality of the hospital reception is very important, it is the first care. Upon his arrival at the hospital, the patient needs information and guidance that must be available at the hospital reception office” (participant ID4). Information at the reception office is supposed to be delivered to patients by specialized and well-informed staff. However, some participants from the patient category reported that they were obliged to ask for information and guidance from the security agents because there was no reception staff. This led to patient dissatisfaction as the information was incomplete.
- Signs and hospital architecture
Inside the hospital, accessibility of care requires the existence of clear signs to locate, inform, and guide the patient through the hospital. All the interviewees recognized the importance of signs to ensure smooth patient flow. Signs allow patients to reach their destinations easily and quickly. Moreover, the fluidity and ease of circulation also depend on the architecture of the hospital “even with the existence of clear signs, patient circulation remains difficult because of the architectural complexity” (participant ID4). From the participants’ point of view, the architecture of the healthcare facility should take into account both the movements of patients and staff to minimize their efforts and reduce the risks of contamination. For example, one of the participants points out that an inappropriate architecture could influence the patients’ health status “after a surgical operation, the patient is transported on stretchers for long distances to reach their room. However, in this case, the patient’s health requires the minimum of movement to avoid post-operative complications” (participant ID2).
- Availability of human resources
Patients’ medical care requires the availability of adequate human resources, in terms of quality and quantity. In this study, all the participants revealed an insufficient number of physicians and nurses ” the number of doctors is very small compared to the number of patients. We were many in the waiting room, and there was only one doctor who has to treat everyone” (participant ID10); ” for some specialties, we have only one specialist. When the latter gets sick or takes his leave, we face serious problems” (participant ID2).
- Availability of material resources
The availability of sufficient and functional material resources (drugs, medical supplies, technical equipment, etc.) is critical to receiving care and satisfying patients “it irritates me when my appointment day arrives and I discover that my appointment has been canceled because of material unavailability” (participant ID8). From the participants’ point of view, the unavailability of material resources can be due to several factors such as dependence on other stakeholders. For example, the drug supply is carried out by the Ministry of Health, and the maintenance of technical equipment is managed through outsourcing contracts. Consequently, the availability of material resources depends on these stakeholders “when equipment breaks down, it is necessary to wait, between few days and several weeks, for the arrival of the repair company” (participant ID3).
- Waiting time
The waiting time dimension includes the time it takes to obtain an appointment and the waiting time on site for consultation, medical analysis, and radiological examinations. All participants agreed that waiting times are critical for both quality of care and patient satisfaction “one more day would have a negative impact on the patient’s health and well-being. Sometimes, the patient’s case requires simple medical interventions if he/ she is treated on time. On the other hand, if he/ she waits several days before receiving care, his/ her health status may get worse” (participant ID2); “waiting times are the major disaster in public hospitals. In my case, I had to wait more than 5 months to get an appointment, and on the day of the appointment, I stayed in the waiting room for 5 hours before seeing the doctor” (participant ID8).
The main cause of waiting times revealed by the participants is the imbalance between capacity and demand. Capacity refers to the available human and material resources, and demand refers to patients’ flow. Another reason cited for waiting times is the non-compliance with the gatekeeping system. Actually, the patient pathway should begin at basic healthcare centers, then provincial and regional hospitals and finally university hospital centers. The non-compliance with this pathway increases healthcare demand and causes long waiting times.
- Consultation time
Participants stated that the longer the consultation time, the more satisfied the patient is. In addition, they have linked consultation time to the quality of medical diagnosis “long consultation times are synonymous with good medical decision-making” (participant ID5); “long consultation times give rise to in-depth discussions with patients, which makes it possible to accurately identify symptoms and signs of disease” (participant ID2). Some participants from the patient category stated that they have not been given sufficient information during the care process because the consultation time was short “the doctor had not given me enough time, he was fast. I left the hospital without understanding what I am suffering from” (participant ID9).
Participants explained the reduction of consultation time in different ways. Some have linked it to the workload “doctors are too busy, they have very long patient queues, so they do not have enough time to examine each patient thoroughly” (participant ID5), and to the caregivers’ performance of non-professional tasks, such as organizing patient records and regulating the queue. Others have associated short consultation time with the lack of motivation “I insist much more on the lack of motivation because the salary is fixed and is not proportional to the work” (participants ID1).
4.3.4. Hospital hotel services
Hospital hotel services refer to the accommodation conditions of patients in hospitals. They include cleanliness, laundry, catering, and comfort during the hospital stay. While discussing hospital hotel services, participants have notified the important role of outsourcer companies because most of these activities are outsourced. The number of coded references corresponding to the hospital hotel services is given in Figure 3.
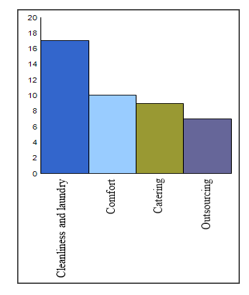 Figure 3: Hospital hotel services – number of coding references per element
Figure 3: Hospital hotel services – number of coding references per element
Participants confirmed that it is essential to pay great attention to hospital hotel services in order to increase patient satisfaction “we concluded, from satisfaction surveys, that patients in some care units such as cardiology are very satisfied because hotel services are good. On the other hand, in hot units such as maternity and emergency departments, patients are dissatisfied, as the hotel services are poor” (participant ID3). For some participants, hotel services in the public hospitals are unsatisfactory, which reduces its attractiveness “I assume that most of the patients prefer private hospitals because of poor hotel services in public hospitals” (participant ID1); “the competitive edge of the health private sector lies in hospital hotel services” (participant ID2).
Hospital cleanliness was consistently mentioned by all participants as a fundamental criterion for the quality of care and safety “cleanliness is very essential because hospitals are full of germs, the risks of contamination are very high. Without cleanliness and hygiene, the hospital would be a place of infection rather than a place of care” (participant ID5). Concerning catering, participants argued that the effective provision of high-quality food is crucial for the well-being of patients. The interviewees revealed a lack of quality and quantity of the served meals. With regard to comfort, participants’ observations focused on the lack of chairs in waiting rooms, lack of air conditioning, room heating, uncomfortable beds, noise during visiting hours, etc.
As hospital hotel activities are outsourced, the outsourcer companies are responsible for facilities maintenance, product supply (food, cleaning products, etc.), production and delivery of meals and clean linen, as well as ensuring the hospital cleanliness, etc. Thus, dysfunctions are attributed to the poor outsourcing management: lack of monitoring and control of service providers, insufficient allocations of staff and products, non-respect of contractual obligations, etc.
- Administrative procedures
Hospital administrative procedures are managed by hospital internal regulations and the Ministry of Health circulars. However, participants from the healthcare professional category reported that these regulations are obsolete and outdated. As for participants from the patient category, they generally expressed their dissatisfaction with the organization of administrative procedures. According to them, dysfunctions are diverse: complexity of administrative circuits, redundancy, lack of clarity and orientation, etc. “the administrative formalities are too complicated; there are a multitude and redundancy of the required documents. In my opinion, all the required documents should be replaced by a single one” (participant ID9); “the procedures are not clear and patients and their families are victims of comings and goings” (participant ID8). In particular, we noted that participants repeatedly raised issues of the RAMED (Medical Assistance Scheme for the Economically Underprivileged), which is a health insurance regime for the poor and vulnerable population. They reported that the RAMED procedure is cumbersome and results in a slow and lengthy care process. When we asked healthcare professionals about RAMED procedure issues, they argued that these dysfunctions stem from patients’ non-compliance with the gatekeeping system. However, for patients, the non-compliance with the gatekeeping system is due to a lack of guidance and difficulties in access to information.
All participants proposed to ease the administrative procedures by simplifying them and reducing redundancies, as well as through the use of Information & Communication Technology. Thus, would reduce the administrative burden and patient’s frustration “in my opinion the best way to overcome administrative documents redundancy problem is to use computerized and electronic procedures” (participant ID3).
5. Discussion
Quality of care is a major issue for healthcare facilities that they are required to improve in order to comply with standards and to meet patients’ needs [38]. Patient satisfaction is one of the important indicators of quality of care. According to previous studies, patients focus on tangible aspects of healthcare services and their administration to assess the quality of care, as they lack the necessary skills to judge the technical quality [39]. Satisfaction surveys revealed a variety of factors that influence patient satisfaction. In this exploratory study, we focused on the following logistics factors: physical accessibility, waiting time, consultation time, hospital hotel services, and administrative procedures. These factors were covered during semi-structured interviews with health professionals and patients from the public health sector in Morocco. The results highlighted the importance of the studied logistics factors for quality and patient-centered care. All study participants emphasized the critical aspect of hospital logistics in accessing healthcare and the management process from admission to discharge.
According to the results, the physical accessibility of healthcare is the logistics factor most often raised by the interviewees. This can be explained by the scope of the elements it includes e.g. location of the healthcare facility, medical transportation, availability of human and material resources, etc., but also by the difficulties encountered by patients in accessing healthcare. Hospital logistics can help in different ways to mitigate patients’ access to healthcare. For example, Frichi et al. [40] proposed to improve medical patient transportation in Morocco by increasing the availability of ambulances through collaborative practices in the healthcare supply chain. El Oualidi et al. [28], developed a mathematical model to optimize the assignment of nurses to emergency departments in a public hospital in Morocco, and thus improve the availability of nurses in these departments. Ben Kacem et al. [41] have suggested a hybrid algorithm to size needed medical resources in case of a massive influx of patients, so as to save maximum lives. In order to better manage drug provisioning in Moroccan public hospitals, Ibn El Farouk et al. [42] built a decision-making tool to select relevant indicators to better measure and manage the medicines supply chain. In the same context of dealing with pharmaceutical issues, El Mokrini et al. [43] have developed a mathematical model for facility location problems to better locate pharmaceutical warehouses in order to serve all demand points such as hospital and basic healthcare centers and to minimize warehouses’ opening cost.
Long waiting times lead to patient dissatisfaction and can affect their health status. One of the causes of waiting times raised by participants is the imbalance between demand and capacity. This is similar to the findings of Silvester et al. [44]. They assumed that failure to control variation in capacity and demand is the main origin of waiting times. Several works in hospital logistics have proposed actions to reduce waiting times. Indeed, Gupta and Denton [45] proposed to apply industrial engineering and operational research tools to optimize appointment planning. Golmohammadi [46] developed statistical and mathematical models capable of predicting the number of patients coming from the emergency department in order to prepare for their reception in the care units. The objective was to reduce the waiting time for preparing patients’ reception.
The consultation time is considered one of the most essential features of healthcare services. Participants reported the benefits of extended consultation time on both satisfaction and quality of care. Similar results have been highlighted by quantitative surveys that have concluded that the length of time spent with the caregiver is strongly associated with patient satisfaction [47,48]. To increase consultation time, hospital logistics researches propose to decrease the workload of caregivers and increase their availability by freeing them from logistical and administrative tasks (e.g. organization of patient records, stock management in care units, transportation of laboratory tests, etc.). These tasks should be performed by dedicated and trained teams [20,49].
A very strong and recognized association is noticed between hospital hotel services (cleanliness, laundry, catering, comfort, etc.), patient satisfaction and quality of care. Given the tangible nature of hospital hotel services, they are easy to evaluate and to which patients are sensitive. These findings are in line with results from other studies. In fact, Suess and Mody [50], through a quantitative survey, have shown that hotel services in a hospital have a major influence on patients’ well-being. Peters et al. [51] discussed and proved the importance of cleanliness in reducing infections and promoting patient safety and satisfaction. Shirzadi et al. [52] reported that patients and their companions ranked highly the importance of hospital hotel services, which shows that they care about these issues. Their study has considered a large number of hotel services including esthetic of physical space, food services, cleanliness, availability of lifts and other services. Efforts to address and improve these nonmedical activities can have a profound positive impact on patient satisfaction and quality of care.
The last factor discussed in this paper concerns administrative procedures for patient admission, treatment, and discharge. Participants agreed on the decisive effect of administrative procedures on patient satisfaction. These results support previous studies [53]. In Morocco, a patient satisfaction survey conducted in a public hospital showed that more than half of patients (54.2%) found the administrative formalities complicated and 60% of them were not satisfied with the organization of their discharge [54]. The optimization of administrative procedures is necessary to reduce patient frustration and increase fulfillment. The existing procedures should be revised in depth to remove unnecessary and duplicate documents. Also, administrative circuits can be improved through the adoption of information technologies, which would help to reduce circuit redundancies and associated delays. Findings from previous research indicated that e-hospital systems increase clinical quality and enhance patient satisfaction and loyalty [55]. In Morocco, some hospital services use Information & Communication Technology e.g. web-based appointment systems [56]. But these applications are insufficient and not yet widespread.
6. Limitation and future research
This qualitative study explored the importance of hospital logistics factors in quality of care and patient satisfaction from the perspective of patients and healthcare professionals. However, this research has several limitations. It was restricted to a few public hospitals in Morocco and a limited number of participants. Therefore, study findings need to be confirmed by other studies on a larger population, using quantitative data collection methods. In particular, future studies would provide quantitative data on the impact of logistics factors on quality and satisfaction to see which of these factors is more preponderant.
7. Conclusion
Previous studies have stressed the vigorous association between quality of care and patient satisfaction on the one hand, and hospital logistics on the other hand. The aim of this paper was to gain a better understanding, through a qualitative study, of the effect of hospital logistics factors on quality of care and patient satisfaction. To this end, semi-structured interviews were conducted with five patients and five healthcare professionals. The combination of patients’ opinions and healthcare professionals’ opinions was of great value to capture different points of view. Results showed that participants gave considerable importance to hospital logistics factors when discussing quality of care and patient satisfaction. Thus, the hospital’s role is not only to treat the disease but also to provide healthcare services that are easily accessible, delivered on time, in a clean and comfortable environment in order to promote the well-being of patients and other service users. Therefore, it is suggested that healthcare planners and managers pay more attention to hospital logistics activities. Future research could be of great help to deepen and measure the impact of the studied logistics factors on quality and satisfaction in order to provide useful data to hospital managers to be able to make sound decisions and determine which factors need to be improved.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgment
The authors would like to thank the participants for their time and valuable contribution to this research.
- Y. Frichi, F. Jawab, and S. Boutahari, “Elaboration of an association matrix of satisfaction factors in healthcare facilities and hospital logistics activities,” in 2018 International Colloquium on Logistics and Supply Chain Management (LOGISTIQUA), 2018, pp. 32–37.
- Y. Frichi, F. Jawab, and S. Boutahari, “Identification of health system stakeholders in Morocco,” in Proceedings of the International Conference on Industrial Engineering and Operations Management, 2019, no. March 5-7, pp. 1193–1199.
- A. Donabedian, The definition of quality and approaches to its assessment. Volume 1. Explorations in Quality Assessment and Monitoring. 1980.
- Q. Nottingham, D. M. Johnson, and R. Russell, “A multi-year SEM model predicting the impact of behavior attributes on overall patient satisfaction,” Int. J. Qual. Reliab. Manag., 2018.
- D. L. Frosch, “Patient-Reported Outcomes as a Measure of Healthcare Quality,” J. Gen. Intern. Med., vol. 30, no. 10, pp. 1383–1384, 2015.
- Y. Frichi, F. Jawab, and S. Boutahari, “The Mixed-Method 5W2D Approach for Health System Stakeholders Analysis in Quality of Care: An Application to the Moroccan Context,” Int. J. Environ. Res. Public Health, vol. 16, no. 16, p. 2899, Aug. 2019.
- A. Mohd and A. Chakravarty, “Patient satisfaction with services of the outpatient department,” Med. J. Armed Forces India, vol. 70, no. 3, pp. 237–242, 2014.
- K. Park, J. Park, Y. D. Kwon, Y. Kang, and J. W. Noh, “Public satisfaction with the healthcare system performance in South Korea: Universal healthcare system,” Health Policy (New. York)., vol. 120, no. 6, pp. 621–629, 2016.
- T. Verulava, R. Jorbenadze, L. Karimi, B. Dangadze, and T. Barkalaia, “Evaluation of Patient Satisfaction with Cardiology Services,” Open Public Health J., vol. 11, pp. 201–208, 2018.
- S. Waters, S. J. Edmondston, P. J. Yates, and D. F. Gucciardi, “Identification of factors influencing patient satisfaction with orthopaedic outpatient clinic consultation: A qualitative study,” Man. Ther., vol. 25, pp. 48–55, 2016.
- J. Fang, L. Liu, and P. Fang, “What is the most important factor affecting patient satisfaction – A study based on gamma coefficient,” Patient Prefer. Adherence, vol. 13, pp. 515–525, 2019.
- C. Bleustein, D. B. Rothschild, A. Valen, E. Valaitis, L. Schweitzer, and R. Jones, “Wait Times, Patient Satisfaction Scores, and the Perception of Care,” Am. J. Manag. Care, vol. 20, no. 5, pp. 393–400, 2014.
- J. G. R. Howie, M. D. Porter, D. J. Heaney, and J. L. Hopton, “Long to short consultation ratio: a proxy measure of quality of care for general practice,” Br. J. Gen. Pract., vol. 41, no. 343, pp. 48–54, 1991.
- K. Põlluste, R. Kallikorm, K. Meiesaar, and M. Lember, “Satisfaction with access to health services: The perspective of Estonian patients with rheumatoid arthritis,” Sci. World J., vol. 2012, 2012.
- B. Mohamed and N. A. Azizan, “Perceived service quality’s effect on patient satisfaction and behavioural compliance,” Int. J. Health Care Qual. Assur., vol. 28, no. 3, pp. 300–314, 2015.
- H. D. SEVİN, “Hotel Services In Hospitals,” J. Tour. Gastron. Stud., pp. 451–459, 2018.
- Y. Frichi, F. Jawab, and S. Boutahari, “Patient satisfaction factors and their correspondence with hospital logistics activities,” in Proceedings of the International Conference on Industrial Engineering and Operations Management, 2018, pp. 1141–1147.
- I. Ibn El Farouk, A. Talbi, and F. Jawab, “Chaîne logistique hospitalière: définition, état de l’art et pistes d’amélioration,” in CIGIMS, FES/MAROC, 2012.
- F. Jawab, Y. Frichi, and S. Boutahari, “Hospital Logistics Activities,” in Proceedings of the International Conference on Industrial Engineering and Operations Management, 2018, pp. 3228–3237.
- S. Landry and R. Philippe, “How logistics can service healthcare,” Supply Chain Forum An Int. J., vol. 5, no. 2, pp. 24–30, 2004.
- T. Melo, “A note on challenges and opportunities for Operations Research in hospital logistics,” Tech. reports Logist. Saarl. Bus. Sch., no. 2, pp. 1–13, 2012.
- R. Khaldi, A. El Afia, and R. Chiheb, “Forecasting of weekly patient visits to emergency department: Real case study,” Procedia Comput. Sci., vol. 148, pp. 532–541, 2019.
- S. Villa, A. Prenestini, and I. Giusepi, “A framework to analyze hospital-wide patient flow logistics: Evidence from an Italian comparative study,” Health Policy (New. York)., vol. 115, no. 2–3, pp. 196–205, 2014.
- B. A. Ahmad, K. Khairatul, and A. Farnaza, “An assessment of patient waiting and consultation time in a primary healthcare clinic.,” Malaysian Fam. physician Off. J. Acad. Fam. Physicians Malaysia, vol. 12, no. 1, pp. 14–21, 2017.
- F. Lerebours et al., “Satisfaction des patientes traitées par chimiothérapie en hôpital de jour pour un cancer du sein: résultats de l’enquête TemporELLES,” Bull. Cancer, vol. 102, no. 4, pp. 316–323, 2015.
- M. Beaulieu, “Une expérience de collaboration logistique,” Gest. Hosp., no. 585, pp. 211–214, 2019.
- S. Landry and M. Beaulieu, “The Challenges of Hospital Supply Chain Management, from Central Stores to Nursing Units,” in Handbook of Healthcare Operations Management – Methods and Applications, vol. 184, Springer, Ed. New York, 2013, pp. 465–482.
- M. A. El Oualidi, J. Saadi, and A. Bellabdaoui, “Problème d’affectation des infirmières: un état de l’art et modélisation. Cas du service des urgences de l’hôpital Ibn Roch de Casablanca,” in Congrès International en Génie Industriel et Management des Systèmes (CIGIMS 2012), 2012.
- S. Chougrani and S. Ouhadji, “Les questionnaires de sortie et la place des usagers dans le projet qualité à l’Etablissement hospitalier universitaire d’Oran,” Sante Publique (Paris)., vol. Vol. 26, no. 4, pp. 499–508, 2014.
- WHO, Essential Environmental Health Standards in Health Care. Geneva, 2008.
- T. Schoenfelder, J. Klewer, and J. Kugler, “Determinants of patient satisfaction: A study among 39 hospitals in an in-patient setting in Germany,” Int. J. Qual. Heal. Care, vol. 23, no. 5, pp. 503–509, 2011.
- L. Zemour, A. Belghitri, I. Damouche, K. Reguieg, R. Tedjani, and N. Midoun, “Mesure de la satisfaction des utilisateurs du dossier électronique médical au sein du système d’information hospitalier à l’établissement hospitalier et universitaire d’Oran, Algérie,” Rev. Epidemiol. Sante Publique, vol. 64, p. S260, 2016.
- L. Kohn and W. Christiaens, “Les méthodes de recherches qualitatives dans la recherche en soins de santé: apports et croyances,” Reflets Perspect. la vie économique, vol. LIII, no. 4, pp. 67–82, 2014.
- G. Imbert, “L’entretien semi-directif: à la frontière de la santé publique et de l’anthropologie,” Rech. Soins Infirm., no. 3, pp. 23–34, 2010.
- W. C. Adams, “Conducting Semi-Structured Interviews,” in Handbook of Practical Program Evaluation: Fourth Edition, K. E. Newcomer, H. P. Hatry, and J. S. Wholey, Eds. New Jersey, USA: John Wiley & Sons, 2015, pp. 492–505.
- V. Braun and V. Clarke, “Qualitative Research in Psychology,” Qual. Res. Psychol., vol. 3, no. 2, pp. 77–101, 2006.
- J. Saldaña, The Coding Manual for Qualitative Researchers – Second Edition. SAGE, 2013.
- E. A. Al-Shdaifat, “Implementation of total quality management in hospitals,” J. Taibah Univ. Med. Sci., vol. 10, no. 4, pp. 461–466, 2015.
- T. S. Dagger and J. C. Sweeney, “Service quality attribute weights: How do novice and longer-term customers construct service quality perceptions?,” J. Serv. Res., vol. 10, no. 1, pp. 22–42, 2007.
- Y. Frichi, A. Ben Kacem, F. Jawab, O. Kamach, and S. Chafik, “Improving Interhospital Medical Patient Transportation in Morocco: A Forcasting Collaborative Approach,” in Transportation, Logistics, and Supply Chain Management in Home Healthcare: Emerging Research and Opportunities, J. Euchi, Ed. Pennsylvania, USA: IGI Global, 2020, pp. 136–162.
- A. Ben Kacem, O. Kamach, S. Chafik, and M. Ait Hammou, “A hybrid algorithm to size the hospital resources in the case of a massive influx of victims,” Int. J. Electr. Comput. Eng., vol. 10, no. 1, pp. 1006–1016, 2020.
- I. Ibn El Farouk, A. Talbi, and F. Jawab, “Development of a Set of Indicators to Manage Medicines Supply Chain in Moroccan Public Hospital , Application of the SCOR Model,” Int. J. Bus. Dev., vol. 3, no. 3, pp. 147–158, 2013.
- A. El Mokrini, Y. Boulaksil, and A. Berrado, “Modelling facility location problems in emerging markets: The case of the public healthcare sector in Morocco,” Oper. Supply Chain Manag., vol. 12, no. 2, pp. 100–111, 2019.
- K. Silvester, R. Lendon, H. Bevan, R. Steyn, and P. Walley, “Reducing waiting times in the NHS: is lack of capacity the problem?,” Clin. Manag., vol. 12, no. 3, pp. 105–109, 2004.
- D. Gupta and B. Denton, “Appointment scheduling in health care: Challenges and opportunities,” IIE Trans., vol. 40, no. 9, pp. 800–819, 2008.
- D. Golmohammadi, “Predicting hospital admissions to reduce emergency department boarding,” Int. J. Prod. Econ., vol. 182, pp. 535–544, 2016.
- J. Ogden et al., “‘I want more time with my doctor’: a quantitative study of time and the consultation,” Fam. Pract., vol. 21, no. 5, pp. 479–483, 2004.
- N. Puri, A. Gupta, A. K. Aggarwal, and V. Kaushal, “Outpatient satisfaction and quality of health care in North Indian medical institute,” Int. J. Health Care Qual. Assur., vol. 25, no. 8, pp. 682–697, 2012.
- S. Landry and M. Beaulieu, “La logistique hospitalière: un remède aux maux du secteur de la santé?,” Gestion, vol. 26, no. 4, pp. 34–41, 2002.
- C. Suess and M. A. Mody, “Hotel-like hospital rooms’ impact on patient well-being and willingness to pay: An examination using the theory of supportive design,” Int. J. Contemp. Hosp. Manag., vol. 30, no. 10, pp. 3006–3025, 2018.
- A. Peters, J. Otter, A. Moldovan, P. Parneix, A. Voss, and D. Pittet, “Keeping hospitals clean and safe without breaking the bank; summary of the Healthcare Cleaning Forum 2018,” Antimicrob. Resist. Infect. Control, p. 132, 2018.
- S. M. Shirzadi, P. Raeissi, A. A. Nasiripour, and S. J. Tabibi, “Factors affecting the quality of hospital hotel services from the patients and their companions’ point of view: A national study in Iran,” J. Res. Med. Sci., vol. 21, 2016.
- F. Canoui-poitrine, H. Logerot, and M. Frank-soltysiak, “Évaluation de la satisfaction des professionnels et des patients d’une unité multidisciplinaire de chirurgie ambulatoire,” Prat. Organ. des Soins, vol. 39, no. 4, pp. 323–330, 2008.
- K. Amazian, I. Toughrai, N. Benmansour, S. A. Laalim, M. E. A. El Alami, and K. Mazaz, “Enquête de satisfaction des patients atteints de cancer dans un hôpital universitaire au Maroc,” Sante Publique (Paris)., vol. 25, no. 5, pp. 627–632, 2013.
- F. Kitsios, S. Stefanakakis, M. Kamariotou, and L. Dermentzoglou, “E-service Evaluation: User satisfaction measurement and implications in health sector,” Comput. Stand. Interfaces, vol. 63, pp. 16–26, 2019.
- S. Bensbih, O. Bouksour, and S. Rifai, “On line appointment systems in a patient Centric Strategy: A qualitative approach in a case study for hospitals in Morocco,” 6th Int. Conf. Control. Decis. Inf. Technol. (CoDIT 2019), pp. 1735–1739, 2019.
Citations by Dimensions
Citations by PlumX
Google Scholar
Scopus
Crossref Citations
- Youness Frichi, Fouad Jawab, Said Boutahari, "Diagnosis of the main issues of extra-hospital medical patient transportation: Case of Morocco." In 2020 IEEE 13th International Colloquium of Logistics and Supply Chain Management (LOGISTIQUA), pp. 1, 2020.
- Ed-Douichi Kaoutar, Jawab Fouad, Frichi Youness, "Unveiling Medical Transportation Problems: extra-hospital, inter-hospital and intra-hospital challenges." In 2024 IEEE 15th International Colloquium on Logistics and Supply Chain Management (LOGISTIQUA), pp. 1, 2024.
- Youness Frichi, Fouad Jawab, Lina Aboueljinane, Said Boutahari, "Development and comparison of two new multi-period queueing reliability models using discrete-event simulation and a simulation–optimization approach." Computers & Industrial Engineering, vol. 168, no. , pp. 108068, 2022.
- Youness Frichi, Fouad Jawab, Lina Aboueljinane, Abderrahman Benkacem, "Maintenance Strategy Selection based on Medical Equipment Prioritization." In 2024 IEEE 15th International Colloquium on Logistics and Supply Chain Management (LOGISTIQUA), pp. 1, 2024.
- Fatima Zahra Benbrahim, Youness Frichi, Abdelhay Benabdelhadi, Fouad Jawab, "The Qualitative Exploratory Study." In Data Collection and Analysis in Scientific Qualitative Research, Publisher, Location, 2024.
- Abdramane Traoré, Hicham Abbad, "The contribution of logistics to improving health care quality: a case study approach." Supply Chain Forum: An International Journal, vol. , no. , pp. 1, 2024.
- Manal El Yadari, Imane Moufad, Fouad Jawab, Jabir Arif, "Logistic 4.0 Implementation For Efficient Urban Freight Transport: A Systematic Literature Review." In 2024 IEEE 15th International Colloquium on Logistics and Supply Chain Management (LOGISTIQUA), pp. 1, 2024.
- Abderrahmane Benkacem, Oualid Kamach, Samir Chafik, Youness Frichi, "Supervised machine learning to allocate emergency department resources in disaster situations." In 2022 14th International Colloquium of Logistics and Supply Chain Management (LOGISTIQUA), pp. 1, 2022.
- Youness Frichi, Lina Aboueljinane, Fouad Jawab, "Using discrete-event simulation to assess an AHP-based dynamic patient prioritisation policy for elective surgery." Journal of Simulation, vol. 19, no. 1, pp. 39, 2025.
- Imane Ibn El Farouk, Imane Moufad, Youness Frichi, Jabir Arif, Fouad Jawab, "Proposing a Supply Chain Collaboration Framework for Synchronous Flow Implementation in the Automotive Industry: A Moroccan Case Study." Information, vol. 11, no. 9, pp. 431, 2020.
- Abdelaziz Zerka, Fouad Jawab, "Critical Analysis of the Evolution of Methods for Calculating Costs of Patient-Centered Health Services." In Hospital Supply Chain, Publisher, Location, 2024.
- Hanane Halimi, Fouad Jawab, Ahmed Bouklata, Frichi Youness, "Hospital logistics based on blockchain: A literature review." In 2024 IEEE 15th International Colloquium on Logistics and Supply Chain Management (LOGISTIQUA), pp. 1, 2024.
- Imane Tronnebati, Fouad Jawab, Jabir Arif, "Innovative Practices for Eco-Friendly Suppliers in the Automotive Industry." In Eco-Logistics and Sustainable Supply Chain Innovations, Publisher, Location, 2024.
- Youness Frichi, Fouad Jawab, "Simulation Optimization Models for Reducing Inequities in Ambulance Coverage." In Hospital Supply Chain, Publisher, Location, 2024.
- Youness Frichi, Fouad Jawab, Lina Aboueljinane, Abdelaziz Zerka, Abderrahmane Benkacem, "Assessing and improving ambulance coverage in the prefecture of Fez using discrete-event simulation." In 2022 14th International Colloquium of Logistics and Supply Chain Management (LOGISTIQUA), pp. 1, 2022.
No. of Downloads Per Month
No. of Downloads Per Country